
































A couple of years back, the following question was sent in to CYC-NET
by someone who had obviously
been hearing a lot about “relationships”
from his Child and Youth Care friends.
I keep hearing so much about the centrality of “the relationship” in the work of Child and Youth Care friends. Are they for real — or is this a bit sentimental and bogus? Surely the doctor and the plumber and the auto repairman must equally have good relationships with their customers/clients/patients? What’s so different with Child and Youth Care people? — Jon (Jack)
The responses he got gave a pretty good review of the concept, but
understandably from “inside” the field (see the entire discussion
archived on CYC-NET, click “The Network” then “INDEX of more discussion
threads”). As someone interested in what might be called “the science of
Child and Youth Care/work,” I wondered what it would be like to try to
answer him more objectively, from “outside” the field.
To do this, I
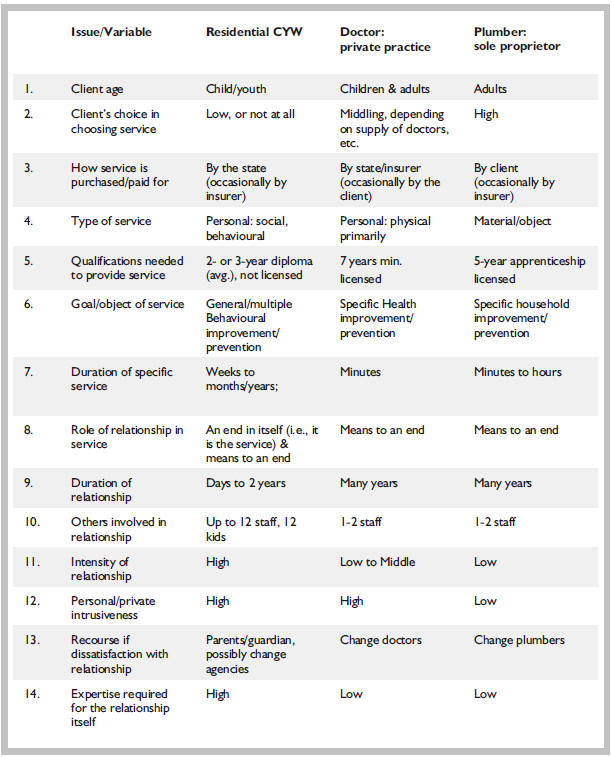
thought a chart comparing the four occupations on some key variables
would be a good place to start. But, before long, it was apparent that
the plumber and auto repairman were quite similar so the repairman was
dropped.
I also made the assumption that Jon, the questioner, had in mind a small plumbing/repair business rather than a large heating-plumbing company or a large auto dealership repair facility, where relationships, if any, are more likely to be with a receptionist or service manager. A single family physician in private practice was chosen for the same reason.
To reduce the need for an exhaustive study of various jurisdictions, I limited the examples to Canada, and Ontario (where I live) where necessary, for example in the “qualifications needed.” So for instance, in the chart below, “the state” or government refers to the province of Ontario, since all three occupations are under provincial jurisdiction. As well, both CYW and medical services are largely paid for by the province but occasionally an insurer will pay for CYW services (e.g., behavioural problems as a result of a car accident) and some extra medical services. Some medical procedures can also be purchased by the client in private clinics.
The “Issue/Variable” items were chosen roughly on the basis of increasing focus on the relationship or interaction itself. So the initial 8 items have to do with the structure in which the relationship takes place – the general service provided – and the remaining items concern the relationship itself within that service.
I then reviewed the responses of those that answered Jon to see how their answers compared with the chart items. A number mentioned one of the basic differences, that the relationship in Child and Youth Care is an end in itself, not just a means to an end (“Role of the relationship in the service”). Also mentioned a number of times was the “Goal/object of the service” (e.g., for the client “to experience real, wholesome, deep relationships,” to learn the “skills of conflict resolution, caring and problem solving” and to “have a fair shot at relating, mutually, with others — without having to bully and dominate”).
The items on “Intensity” and “Personal/private intrusiveness” of the relationship received a fair bit of comment. This generally took the form of almost poetic statements about the nature of “relationship” – “being in the moment,” “a feeling of ‘we’-ness,” “the transformational heart of Child and Youth Care,” and a “’fusion of joint experiencing’.” The negative side of intensity (tantrums, aggression, screaming, stony refusal, etc.) that was so much a part of earlier Child and Youth Care writing (and many CYWs present-day experience) was noticeably absent. Perhaps it was this that led Jon to comment that such talk is “a bit sentimental and bogus.”
The responders’ comments on the intensity of relationships also suggest the kind of “Expertise required for the relationship itself.” The discussants spent some time directly on that, the kind of skills and personal attributes needed to make such transformational connections with children and youth. This, perhaps inevitably, led to a discussion about processes for selecting CYWs. The closest term for this that I could come to in the chart for comparison purposes was “Qualifications needed.”
And it is here that one of the starkest contrasts comes out in the chart, by comparing the plumber with the CYW. The CYW has sustained contact (#7 and #9), with high intensity (#11) and personal intrusiveness (#12), requiring high expertise (at least for the relational part, #14), but only a 2or 3-year diploma is required and no license (#5). The plumber on the other hand requires a license and a 5-year apprenticeship. The conclusion, as a direct answer to Jon, has to be:
A relationship is central to Child and Youth Care, but the plumber’s relationship is much more highly valued by society – it takes 5 years and a license just to enter into the relationship. The implications of this for the need for strong professional Child and Youth Care associations seem to me to be pretty blatant.
The other major contrast coming from the chart jumped out at me within minutes of starting the chart – Item #2.
Again as an answer to Jon, the major difference between doctors/plumbers and CYWs is that CYWs’ clients have little to no choice in entering into the relationship. And to draw the contrast even more sharply, though the relationship is going to be long (#7 and #9), intense, (#11), personal (#12), with probably no way out (#13), the client has no choice. And by the way, it could involve a lot of other (no-choice) relationships (#10), and society doesn’t particularly care (#5).
The implications of this finding from the chart are numerous, enough perhaps to re-open a CYC-NET discussion on relationships. One CYW I showed the chart to saw the need for very specific types of CYWs, ones who would be able to appreciate the control function of Child and Youth Care yet at the same time exercise the caring function. This aspect of the chart made me wonder how much of the behaviour CYWs deal with is the child’s reaction to having little or no control or choice in the matter. It certainly reinforces the position of those who have called for a greater awareness of the child’s sense of what “coming into care” means.
I’m sure there are many other implications to be drawn from this exercise, but for me the major one concerned viewing Child and Youth Care/work as a “science.” If science involves defining concepts in ways that they can be measured and tested – being more objective about our profession – this small attempt at doing so has definitely reinforced my view that such an approach would be well worth pursuing.


