

































A metaphor for crossing a frontier into a new territory is explored. The restorative justice principles as used by the United Nations and IIRP help to translate into restorative practice principles. An action research project in South Africa provides the background to an evaluation process. Prevention and early intervention levels invite practitioners to use the restorative principles in their own daily practices.
Metaphor
The invitation to cross a frontier into a new territory requires certain
knowledge, skills, and experience. Pioneers who travel across the
mainland in search of new territory experience doubt and hardships on
the journey. The new territory poses challenges that invite new ways of
working. Cooperation and co-vision become essential principles of
survival if a new way of living restoratively is to be realized.
Global perspective
Van Rensburg (2004) states that with the growing trend to move toward
globalization of health, health policy and health care, a set of
processes are in place where unprecedented interconnectedness is
blurring a variety of boundaries and transforming the nature of human
interaction across a wide range of spheres. This in turn increases
economic, political, and social interdependence.
In the social service framework where many disciplines have defined their specific ways of intervening, “blurring a variety of boundaries” is threatening. Yet if we are to take the nature of human interaction to heart, boundaries only exist in theory.
Globally in social services, four levels of intervention exist: prevention, early intervention, statutory care, and continuum of statutory care. Each country has variations to these four levels. Prevention and early intervention levels are often handled by the health care and educational systems, whereas statutory and continuum of care levels involve the state and judiciary systems. These theoretical boundaries have been convenient ways of practicing.
Restorative justice
Over the past thirty years, the criminal justice system has been
challenged by pioneers crossing the frontiers of the discipline of
criminal justice and challenging it. Pioneers like Christie (1977),
Braithwaite (1989), McCold (1999), and Zehr (2002) have ventured to
transgress boundaries in their respective disciplines and develop
alternatives to addressing harms. Restorative justice theory and
practice has grown and challenged mainstream thinking and practice.
The culmination of their efforts is evident in the United Nation's adoption and publication of a hand- book on restorative justice definition, processes, and practices. This is held up as a model of good practice.
Three definitions stated in the handbook are:
“Restorative justice programme” means any programme that uses restorative processes and seeks to achieve restorative outcomes.
“Restorative process” means any process in which the victim and the offender, and, where appropriate, any other individuals or community members affected by a crime, participate together actively in the resolution of matters arising from the crime, generally with the help of a facilitator. Restorative processes may include mediation, conciliation, conferencing, and sentencing circles.
“Restorative outcome” means an agreement reached as a result of a restorative process. Restorative outcomes include responses and programmes such as reparation, restitution, and community service aimed at meeting the individual and collective needs and responsibilities of the parties and achieving the reintegration of the victim and the offender. (United Nations, 2007)
Restorative justice principles ask for changes in belief and value systems. The retributive system leaves gaps in reintegrating human beings into society Braithwaite concludes, “while shaming by the state is less potent than by proximate communities, effective state shaming is one of the factors which assist societies to maintain low crime rates” (Braithwaite, 1989, p. 97).
Purpose
For those of us working in health care and education, where prevention
and early intervention are our primary focus, how can restorative
justice definitions be translated into the our everyday milieu?
Referring to these values and principles as restorative practices, how
would the questions we ask of ourselves be different?
Restorative practice principles
How does one invite a restorative paradigm shift into your practice?
Core values and principles of restorative practices make it different
from mainstream practices. Practices like empowerment, cooperation, and
involvement toward the goals of responsibility reparation, and
reconciliation and the development of social competency using
interactional dialogue and fair process are challenges to mainstream
expert knowledge (IIRP Website, 2007).
Restorative practices challenge us to re-story our daily lives and work using five basic principles. These basic principles could be viewed as rivers that need to be crossed in order to reach the new territory. According to the International Institute for Restorative Practices the following principles guide our exploration:
Principle 1: Participation achieved through cooperation rather than coercion. Pivotal to restorative practices is the ability to build relationships within a society where disconnection is becoming the norm rather than the exception (Braithwaite, 1989). This involves respecting and encouraging individuals and communities to participate in their own decision making. Participants take responsibility for their actions and build communities of respect. Inherent respect acknowledges that everyone has knowledge, experiences, and skills that could aid them in making appropriate decisions. Achieving this principle is only possible through respect and building a relationship.
Communities may be defined as family the work- place, a community project, a school, or a conflict. A community is dependent on relationships. If relationship building is continuously mindful of doing things “with” others, knowledge, experiences, and skills will be continually built on within the community The community models the family. Relationships are pivotal to both. The role of shame or social disapproval may be effective within family or community where relationships have been nurtured. Braithwaite (1989) maintains that the restorative justice premise needs a “shame” response to operate if society is to reduce crime effectively Members who are “shamed” or who receive social disapproval seek forgiveness and an apology so as to feel reintegrated with the family or community. The relationship they have with the family or community is important to them.
Principle 2: Face-to-face participation of those directly affected. Harms create needs; needs require responses. lf needs are not met, post-traumatic symptoms are more likely to be created by the body and mind (Strang, 2001). The need to ask questions and seek out explanations for the harm promotes emotional healing. To address the needs created, it is important that participants directly affected join together to provide a space for compassionate witnessing (Weingarten, 2004). (ln restorative practices the use of the word “participants” is preferred rather than victim and / or offender.) In face-to-face interaction, where circles are the common practice, a seated circle requires all participants to be open for discussion. In such a circle, a talking piece is used to indicate who will speak. Other people in the circle respect this process and listen. When the speaker has finished, he or she may pass the talking piece on to the next person. The first person to start speaking also chooses the direction of the circle. The circle process establishes a ritual and pattern that allows all voices to be heard.
Apology may occur more naturally in this setting. Contracts towards reparation are drawn up as a result of the discussion that takes place in the circle. Even a symbolic apology sustains relational connections (McCold, 1999).
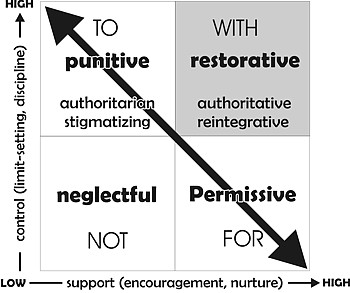
Principle 3: Those directly affected determine the outcome. Allowing those affected by the harm to make decisions that affect them requires professionals to have a belief in the participants. This challenge is not an easy one, since professionals have spent years becoming the “experts.” The social discipline window developed by Wachtel and McCold (2001) provides the cornerstone to restorative practices. (See Figure 1.) Many of us are used to serving others by doing things “for,” “to” or “against” them. Continual awareness and reflection are required to work “with” people.
Social discipline window
The professional’s role is that of a facilitator. Providing the bottom
line to maintain a safe environment with face-to-face participants is
the key objective of the facilitator. Participants and families
determine their own outcome through fair process, where engagement,
explanation, and expectations are common practice (Kim and Mauborgne,
1997). These criteria are needed if participants directly affected are
to determine the outcome.
Figure 1. Social Discipline Window
Principle 4: Fair process includes access and informed consent. Informed consent and access to any documentation needs to be transparent for the family concerned. Due to the highly intimate and emotional nature of the face-to-face interaction, facilitators make the contract a ritual where everyone present signs it. The cathartic experience of participants is a fair process for each voice to be heard.
The invitation of face-to-face circles to discuss the impact of the harm provides space for all persons to be heard without prejudice. Facilitators awareness of dominant, silent, or absent voices is monitored through the use of a talking piece. Voices are heard without backlashes, reprimands or dominant voices monopolizing space. This is not a blaming session. The intent is on how you were affected by the action; how you and others around you were affected by the action; and how amends might be addressed. Sharing how harm affects life’s meaning and purpose propels the conversation to another level of discourse. Respect in maintaining relationships remains the primary focus. lf connection is maintained, reintegration into society is more accessible. It is disconnection that creates stigmatization (Braithwaite, 1989). The use of circle processes and questions provide opportunities for fair process to be achieved (Wachtel and McCold, 2001; White, 1989).
Principle 5: Best practices are demonstrated through our own practice. Each practitioner has the responsibility of reflecting on his or her own practice. When you become a reflective practitioner, you create awareness and empower your own practices. When you enter into this process, you are doing your own action research. Action research requires documentation and reflection of real world experiences that create a meaning and purpose for all participants. Being restorative would ask that you be aware of the above principles in your work. The restorative-reflective practitioner empowers him- or herself with daily awareness activities that enhance the development, repair, or improvement of relationships and strategies where social capital is built through collaborative empowerment. Restorative practices focus on relationships and require engaging with those involved (HRP Website, 2007).
To gain clarity on how restorative principles may be translated into the real world, let us evaluate a reflective action project in South Africa.
Background to action project
“Restory-ing” our restorative practices in an early intervention level
at Mzamo Guidance Clinic (MGC) was the challenge. The MGC is a
non-profit organization working in the Umlazi district, South Africa,
with a population of a million people who have marginalized or limited
social service delivery.
The reality was that the MGC’s referral rate grew, and only four social workers employed with the organization were seeking alternative strategies to assist them in the overload of referral cases. The Education Department’s Psychological Services for Education (PSES) was not offering any educational service to MGC. Since the majority of referrals were from schools that found PSES consultations inadequate for their needs, MGC was seen as a last resort. Durban Institute for Technology (DIT), a university which trains Child and Youth Care practitioners, received and responded to the invitation to visit and review any possibility of potential involvement.
After a visit and in-depth discussions with the MGC, an agreement was made to conduct two pilot studies, each consisting of eight weeks in duration, where a collaborative action project would be conducted.
Purpose of action project
To establish a group decision making process appropriate to the cultural context in MGC;
To use university students currently in their fourth year of studies to address the lack of human resources within the MGC;
To use the professional multi-disciplinary team in the most efficient and effective manner;
To provide real life opportunities for face-to-face interaction where participants directly affected by the harm are able to engage and explain their needs;
To provide university students an opportunity to respond to educational and social harms within the MGC’s referral population using restorative principles.
Preparation of various stakeholders
The university students called a community of professionals to
brainstorm how each could be engaged in a meaningful way to respond to
MGC’s request for assistance in addressing the Umlazi families” needs.
Case one
Mrs. Ngobo* and her 9-year-old son, Sihle, had been waiting for three
years to get into a school that would accept him. Sihle had attended the
local school for one week when his teacher asked Mrs. Ngobo to remove
him, as he was too disruptive in class. Sihle had been injured at birth
with a forceps and carried a large scar on his forehead. Sihle was
mentally challenged. His mother had to keep watch over him continually
as he often endangered himself and other members of the community
through inappropriate risk taking. Mrs. Ngobo was desperate for advice
on where and what to do with her child. She had no idea of her rights
and what resources she could access to help her child. She needed to
travel 75 km to reach MGC, only to find that she must be placed on a
waiting list where no promises could be made due to the overload of
current referrals.
Case two
Another case on the waiting list was Martha, a twelve-year-old girl, who
had left home because her mother scolded her for coming home late every
evening. Martha left home without notifying her mother where she was.
She befriended older men in the community and was exchanging sexual
favors for food treats. The school was aware of her behavior and
contacted Martha’s mother. Her mother asked Martha’s aunt to assist her
in tracking down Martha. The aunt found that she and Martha could talk
and invited Martha to stay with her. The MGC was asked to assist
Martha’s mother in addressing Martha’s behaviors and attitude towards
adults.
These are two examples of the one hundred and sixty cases that were waiting for the MGC’s social workers, with no hope of addressing any of them within the next six months.
The multi-disciplinary team included psychologists from Education Department, (PSES), social workers from MGC, Child and Youth Care students from Durban Institute of Technology (DIT), intern social workers from University of South Africa (UNISA), and occupational therapists from the Education Department. The multidisciplinary team was aware of the time restraints of all the professionals.
A plan was devised that involved DIT Child and Youth Care students as facilitators. In the first phase, DIT Child and Youth Care students received skills training over a period of 12 weeks. The use of restorative circles and questions, using family mapping, conferencing, and family alone time were some of the skills the DIT Child and Youth Care students received (Wachtel and MCold, 2001; Burford, Pennell and MacLeod, 1995).
During the second phase of the plan, DIT Child and Youth Care students met with their families over an eight-week period. During this time, a DIT supervisor was on site and rotated between all the family group meetings that were being conducted. During the seventh week, DIT Child and Youth Care students met with the professionals to share their knowledge of the family with them. During this meeting professionals shared relevant resources and appropriate placement settings with the DIT Child and Youth Care students. DIT Child and Youth Care students discussed the options with the family the following week. At the eighth meeting, families were assisted in drawing up a plan for their young person using the resources that were appropriate and available. The plans were written up by the DIT Child and Youth Care students and given to the parents, MGC, and the PSES to follow through.
Ten families were identified by MGC for each of the two planned pilot studies. The remarkable aspect of both pilot studies showed that all families arrived a few hours before each appointment. Parents showed extreme diligence in meeting their appointment times.
The process that was followed:
Circle interviews were held with the family and a DIT Child and Youth Care student. During this time a family map was developed and developmental strengths and challenges were addressed.
Exploration and conversations with youth and DIT Child and Youth Care students were conducted. Reading, comprehension, and numeracy skills were identified using playful strategies.
A circle discussion on each youth’s case was held where the DIT Child and Youth Care student presented his or her case to the professional group. Options were brainstormed and noted for further discussion with family.
Family circle time was held, in which the DIT Child and Youth Care student provided the family with resources and professional information needed in order to come to a decision. The family was then given time to ask questions.
The family and the DIT Child and Youth Care student drew up developmental plans for the youth with the family. Issues around the four major components of the young person's sense of belonging, mastery, independence, and generosity were addressed. Families were asked how the young person's strengths might be used to address the developmental needs (Brendtro, Brokenleg and Van Bockern, 1990).
Case one
Mrs. Ngobo’s bottom line was to keep Sible safe and maintain contact as
frequently as possible.
The plan adopted was for Mrs. Ngobo to visit the special needs school with Sihle, as suggested by the educational psychologist, and thereafter to meet with the educational psychologist and complete the necessary paperwork for Sihle’s entry into the school. Mrs. Ngobo also scheduled an appointment with the MGC social worker to complete forms for applying for a child dependency grant, to which she was entitled. Sihle would attend a special needs school daily. Transport to and from school could be arranged at the school. Mrs. Ngobo requested a regular time each week to be able to phone and talk to the social worker about ongoing challenges.
Case two
Martha and her mother were asked to come up with a plan for how Martha
could attend school regularly and maintain an evening curfew.
Martha’s aunt and uncle suggested that Martha stay with them she would sign a contract that she would be home at six each evening. Martha agreed to this. Mother agreed to attend basketball matches in which Martha played. Mother also wished to visit her sister once a week and have an hour of special time with Martha. It was agreed that if blaming and shouting began, the visit would be cut short and they would try again the following week. Once the hour visits were achieved without negative moments, it was agreed that Martha would try one weekend at home. The aunt and uncle agreed to let the social worker know by telephone the progress made each week. The social worker would visit Martha every second week and discuss personal hygiene and awareness with regard to sexuality.
Evaluation of using restorative principles
The DIT Child and Youth Care students rated their own practices
and how often they were able to use specific restorative practice
principles. They listed the following issues as pertinent to their
practice. A rating of five meant that they felt they had met the
criteria; a rating of one meant that they fell short of fulfilling a
restorative principle. DIT Child and Youth Care students rated
themselves on key issues thought to relate to the restorative practice
principles.
Conclusions
The action project process revealed three of the five principles being
used consistently in application to the MGC project:
Principle 1. Participation achieved through cooperation rather than coercion. Respect required us to speak as if the people are present all the time, keep appointments that we make, and give a clear understanding of what we expected of the family. Many times this would come in the form of writing a note for the family to have evidence of their visit. This also included respecting their need to speak in their language, e.g., Zulu; introducing ourselves by first names; wearing name tags so as to be identified easily; speaking to the family by being curious and facilitating a process of sharing.
One thread can be broken, but two threads intertwined are more difficult to break. The building of the relationship with the family was visible and strong and made a difference during the process of the eight weeks.
Principle 4. Fair process includes equal access and informed consent. This involved recognizing everyone’s basic human rights and maintaining an awareness of how to fulfill them. Every family had the right to be interviewed in their own language. Where students were able to speak Zulu, we paired them with a Zulu speaking student. The families were entitled to information, procedures, confidentiality, and anonymity. DIT Child and Youth Care students would refer to the young person by their initials in their Individual Developmental Plan (IDP); parents were given an IDP with all the relevant information in it. DIT Child and Youth Care students were expected to keep the young person's file updated with information. These procedures allowed students to maintain accountability each time a young person was interviewed. Transparency was necessary at all times so that other professionals dealing with the case were informed and could follow up on the case.
The DIT Child and Youth Care students presented each individual case, worked with professionals, and discussed possibilities for drawing up an IDP. This rich sharing of potential and possibilities provided students with insights into complex human needs. This never could have been achieved if we had not had the professionals in the process. Thereafter, the DIT Child and Youth Care students invited each family to a discussion of the possibilities that were available for their young person. Families left with a copy of the recommendations. Follow-up work was done by social workers at the MGC.
Principle 5. Best practices are demonstrated through our own practice. Celebrating diversity by engaging with the people across disciplines prepares students for differences. DIT Child and Youth Care students voluntarily devoted time beyond the requirements. Their feedback on how they experienced working in this solution-focused learning process encouraged time to integrate theory with practice. Regular group debriefing was an essential ingredient for intern students and professionals. Reflective practitioners will continually ask the question “How?” in their practice. Time for reflection and conversation was purposefully built into interview time.
Two areas that DIT Child and Youth Care students found the need to rethink and adapt their restorative practice principles were Principles 2 and 3.
Principle 2. Face-to-face participation of those directly affected. The restorative aspects were that students engaged in fair process with families. They were actively engaged with their families, gave explanations and clarified expectations with the families. The relationship building was intense and provided students with hands-on experience to develop family maps and connections. The DIT Child and Youth Care students were able to engage individually with the child or youth in playful reading, numeracy, and comprehension activities and experience some of the individual needs of each young person.
Aspects that did not fulfill the restorative principles were that all participants who were directly affected were not able to attend the circles. Reasons for this varied from financial restraints, work commitments, and no available relatives.
Principle 3. Those directly affected determine the outcome. Creating private family time did not happen. Burford, Pennell, and MacLeod (1995) suggest that families have time alone after professionals have advised on possible resources and provided the bottom line requirements that are needed to keep the young person safe. This is important if families are to take responsibility for the outcome. ]oint discussions were held with the family but no time alone was allowed. However, the families in the MGC project left with a sense of having contributed to their own plan for their young person.
The purpose of the action project was achieved, with high value placed on the role of the university student learners as insightful facilitators. We established a group decision making process appropriate to the cultural context in MGC and used university students to address the lack of human resources within the Mzamo Guidance Clinic.
The use of the professional multi-disciplinary team in the most efficient and effective manner enabled professionals to spread their expertise to a wider base.
The two pilot studies show how connecting across various disciplines may blur boundaries but supports the needs of children and youth in marginalized communities in a far more dynamic and real way.
The pilot study provided real life opportunities for face-to-face interaction where participants directly affected by the harm are able to engage and explain their needs. Fifteen of the twenty children and youth were experiencing unresolved grieving processes coupled with either learning problems and / or severe mental challenges. It was only when the child or youth displayed acting out behaviors, aggression, or high levels of distractibility that they were noticed. Relational support, where emotional and social skills are role modeled, were lacking in all cases. This provided university students” an opportunity to respond to educational and social harms within the Mzamo Guidance Clinic’s referral population and work “with” families to reach a solution for which families took ownership.
Restorative practices invites the character of societal institutions, groups, processes, people, places, and programs to work with social conflict, including the prevention or early intervention levels of harmful behavior and injustices. The challenge to become an advocate and daily practitioner of restorative practices is a new frontier. Crossing new frontiers requires periods of doubt. Using daily reflection and evaluating personal practices using guidelines as described in the evaluation grid may clarify one’s purpose and dispel doubt.
This invitation is for you to “restory” your
practice.
*Note: Names have been
changed to protect the families.
References
Braithwaite, J. (1989). Crime, shame and reintegration. New York. Cambridge University Press.
Brendtro, L K., Brokenleg, M. and Van Bockern, S. (1990). Reclaiming youth at risk: Our hope for the future. Bloomington, IN. National Educational Service (Solution Tree).
Burford, G., Pennell, J. and MacLeod, S. (1995). Manual for coordinators and communities: The organization and practice of family group decision making. Saint ]ohn's, Newfoundland, Canada. Memorial University of Newfoundland, School of Social Work, Family Group Decision Making Project.
Christie, N. (1977). Conflict as property. The British journal of Criminology, 17, 1. pp. 1-14.
IIRP Website (2007). http:/ /www.iirp.org. IIRP Academic Defnitions.
Kim, W. C. and Mauborgne, R. (1997). Fair process: Managing in the knowledge economy. Harvard Business Review, 75, 4. pp. 65-75.
McCold, R. (1999). Restorative justice practice: The state of the field 1999. Paper presented at the Building Strong Partnerships for Restorative Practices conference, Burlington, Vermont.
Strang, H. (2001). Justice for victims of young offenders: The centrality of emotional harm and restoration. In G. Maxwell and A. Morris (Eds.). Restorative justice for juveniles (pp. 183-193). Oxford. Hart Publishing.
United Nations. (2007). Handbook on Restorative justice Programmes. New York. Author.
Van Rensburg, H. C. J. (Ed.). (2004). Health and Health Care. Pretoria. Van Schaik Publishers.
Wachtel, T. and McCold, P. (2001). Restorative justice in everyday life. In J. Braithwaite and H. Strang (Eds.). Restorative justice in civil society (pp. 117-125). New York. Cambridge University Press.
Weingarten, K. (2004). Witnessing the effects of political violence in families: Mechanisms of intergenerational transmission and clinical interventions. Journal of Marital and Family Therapy, 30, 1. pp. 45-59.
White, M. (1989). The externalizing of the problem and the re-authoring of lives and relationships. Dulwich Centre Newsletter, 3, 20. pp. 5-28.
Zehr, H. (2002). The little book of restorative justice. lntercourse, PA. Good Books.
This feature: Rundell, F. (2007). “Re-story-ing” our restorative pratices. Reclaiming Children and Youth, 16, 2. pp. 52-59.