

































Our experiences with the Circle of Inclusion Project (CIP) at the University of Kansas have contributed to our interpretations of the issues facing families with infants, toddlers, and preschoolers who are just beginning to learn about the formidable barriers of an enormous and complex system.
We do not really believe we are writing about “children who challenge the system.” Instead we believe that we are writing about little children and their families who are challenged by the system – a system that is frequently unresponsive, often demeaning, sometimes rejecting, and occasionally cruel.
This chapter includes stories about children, results based on systematic data collection, and programmatic outcomes as well as reflections about our shared experiences over a 10-year period. All that we have to share is supported by rich empirical and theoretical literature about developmentally appropriate early childhood practices, effective early childhood special education practices, integration of children with and without disabilities, the roles of families in early childhood services, the value of the collaborative process, and issues of system change.
This knowledge has now become “our knowledge” in the sense that it has evolved over time as a result of direct engagement with children, families, personnel, and programs in restructuring inclusive early childhood services for young children with significant disabilities and their families. Theories, principles, and practices acquired their meaning through genuine and prolonged engagement with the process we sought to understand.
In keeping with other discussions of CIP (Thompson, Wickham, Ault et al., 1991; Thompson, et. al, 1993), the first section of this chapter, Children and their Families: Stories of Our Pathfinders, describes some of the children and families we have known through out work. The next section, Our Work and Our Values, provides an overview of the values, history, and activities of CIP. Our Knowledge About Knowledge: A Summary of Results and Outcomes, summarizes our strategies for understanding the process with which we have been associated and blends program outcomes, results of studies, and our experiences into thematic topics. The last section, Final Comments and Recommendations: Features of an Exemplary Program, offers a brief overview of the elements that we believe emerged as important for early childhood services for young children who “challenge the system.”
CHILDREN AND THEIR FAMILIES: STORIES OF OUR PATHFINDERS
We are including stories of the children we have worked with and their families because it was these children and their families – stories that taught us the most. With much difficulty we selected three children, Dana, Ashley, and Sheronda to illustrate important aspects of our experience.
Dana: The First Child
At the time of this writing, Dana is a sixth grader in an elementary
school in Lawrence, Kansas.
We met Dana, the first child in the program that was to evolve into CIP,
when she was 3 years old.
Dana is a beauty with enormous brown eyes, thick dark hair, olive skin,
and a warm smile that speaks directly to the heart. She has multiple
disabilities, including mental retardation, spastic quadriplegia with
very limited head control, and no ability to walk, sit unsupported, or
speak. The quality of her vision is not known. These remarks reflect our
earliest memories of Dana: 2
When I met Dana she was three years old. She was lying on a mat in an
overcrowded day room of an institution surrounded by people of all ages
(mostly adults) with profound disabilities. The room was crowded and
filled with the sounds and smells that occur when persons with profound
mental retardation, significant physical disabilities, and serious
medical conditions are crowded together in a sterile, under-staffed,
hospital-like environment in a state institution. The only speaking
voices came from a large TV bolted to the wall about eight feet above
the floor. (Thompson, Wickham, Ault, et. al., 1991, p. 12)
Shortly after my visit I found myself thinking about my three year old granddaughter, Chelsea, and about the marked differences in Dana’s and Chelsea’s daily life experiences. A quotation which has been attributed to Nicholas Hobbs came to my mind. “All children should know joy.” From where was Dana’s opportunity to know joy to come? (Thompson, 1994, p. 3)
Within several months, Dana was welcomed into a wonderful foster family in Lawrence, Kansas, community. Consequently, in the fall of 1986, we were looking for a community-based early childhood program whose staff would be willing to accept Dana. Initially there was no space in a special education preschool classroom, nor did the program accept children with severe multiple disabilities. Her foster parents believed (as did we) that it was important for Dana to have opportunities to be around other children and to be involved in preschool activities away from her foster home for a portion of the day.
We decided to contact one of the most respected programs in the community, Raintree Montessori School, a program that always has a long waiting list of children whose families are seeking early childhood education and child care. When we called Raintree, we began with a description of Dana. We also explained that a university student interested in the integration of preschoolers with disabilities would be available to assist Dana’s Montessori teacher in meeting Dana’s special needs and to enhance the adult-to-child ratio while Dana was in the classroom.
I was half expecting to be turned down and certainly assumed that I needed to do a real “sales” job on why Raintree staff might want to consider accepting a child like Dana. As long as I live, I will never forget Pam Shanks' answer, “Lleanna McReynolds, our Program Director, and I are so excited you thought of us! We would love to have Dana. When would you like for her to start?”
Just a few months later when I first saw Dana in Raintree Montessori School, her presence in this children's house was in such marked contrast with my memory of Dana in the institution that it evoked one of the most emotional experiences of my life. Dana looked valued, respected, and at home surrounded by other preschoolers who accepted her as one of them – which, of course, she was. (Thompson et. al., 1993, p. 13)
Ashley: the “Dignity of Risk"
Ashley is a 6-year-old kindergartner. She is large for her age and quite
striking. She wears her
black curly hair in a braid pulled to the side with a bright ribbon. Her
face is round and pretty with dark eyes and long lashes that accentuates
her soft brown skin. We first knew her as a 2-year-old who had just
suffered a spinal cord injury in a car accident in which she was a
passenger without a seat belt. After months in a pediatric intensive
care unit in which she was termed a “miracle child” for surviving such a
significant injury, she returned home with full paralysis beginning at
the first cervical vertebrae, a permanent tracheotomy, a respirator for
assisted breathing, and a button gastrostomy.
Initially Ashley received home services from an early intervention
program in which therapists
and an early childhood special education teacher worked directly with
Ashley, her mother, and a
nurse. During her third year, Ashley’s mother expressed a strong
interest in having her attend preschool with other children. During the
next 2 school years, she was placed in an excellent preschool located in
an elementary public school building funded through Elementary and
Secondary Education Act (ESEA), Chapter 1. She also attended a private
Montessori preschool during the intervening summer. Ashley began by
spending less than a full session for a few days a week. Within the
first year, her attendance was increased to the full daily for all 5
days per week.
Ashley brought with her the challenges of a medically complex condition
and very significant
physical disabilities. Fears about caring for Ashley were common across
special education and general early childhood staff. Concerns were
related to her breathing, suctioning procedures, and management of the
range of physical problems associated with her condition. What was not a
challenge was finding understanding peers who welcomed her into the
classroom and, with some adult guidance, made the accommodations in
their play needed to include her in activities.
We became used to pointing out that if Ashley was too fragile to be in
an inclusive preschool
classroom, she was too fragile to be in a special education classroom.
Because there were risks for
Ashley associated with her participation in a preschool program, some
medical personnel has recommended she remain at home with 24-hour
nursing care. Her mother’s decision to involve her in an inclusive early
childhood program was based on a commitment for Ashley to be an active
participant in life. Ashley’s participation taught the involved staff
(teachers, therapists, paraprofessionals, and nurses) much about
revising traditional beliefs about roles and responsibilities as well as
about establishing consistent, reliable medical and emergency procedures
within the context of a preschool classroom. Most important, it once
again reminded those around Ashley of the importance of her right to be
a child and to know joy.
Sheronda: From Medical Center to Kindergarten
Sheronda is currently doing well in a multi-age inclusive classroom for
5-, 6-, and 7-year-old
children in an elementary building. She has a number of friends, several
best friends, and a very best friend, Matt. While she still challenges
her teachers to provide positive behavior supports, Sheronda is starting
to talk quite a lot and is learning to read and write. When we first met
Sheronda, she was a cute 3-year-old who participated in a self-contained
special education preschool for children with autism that was housed
within a university medical center. There were four children in the
classroom, which was staffed by a teacher and two assistants.
Sheronda was nonverbal and had a number of challenging behaviors. One of
her most problematic behaviors was running away. She was easily provoked
into major tantrums when asked to comply or when a change occurred in a
routine or in the environment. Sheronda sometimes attacked the other
children by biting and slapping without obvious provocation.
During her second year in preschool, when Sheronda was 4, her program
was moved from the
medical center. She and her three classmates were placed in different
inclusive preschool programs, and their teacher supported the teachers
in these programs. Special education and related services were offered
on a collaborative/consultative basis, and an additional
paraprofessional with specialized training was added to each of the
classrooms the children attended. The program in which Sheronda was
placed offers full-day child care, which met important needs for her
working mother and father. Despite these facts, there was a considerable
concern about her placement in this preschool classroom of 18 children.
Her very challenging behavior and quick exits from home and classroom
were viewed as major threats to a successful outcome.
The initial period of adjustment to this program was a stressful time
for Courtney, Sheronda's
early childhood special education teacher. It was a difficult transition
from being the lead teacher
with four beautiful children in her own classroom within a prestigious
medical center to serving as an itinerant and collaborative teacher with
four different early childhood teachers in community-based early
childhood classrooms. Courtney likes to recall an early transformational
experience when she entered Sheronda’s classroom and was unable to find
her. Courtney remembers her feeling of utter panic in her certainty that
Sheronda had escaped the confines of the classroom and was wondering
around the center or the urban neighborhood. She approached the
classroom teacher, who calmly pointed to a small group of children
building with blocks. Courtney looked intently at the children and
suddenly realized that Sheronda was one of them:
It astounded me, because she blended into the group so well. It wasn’t really that she was cooperatively involved with the children, but she
was engaged and very near the children. She looked just like one of
them. My eyes filled with tears until, once again, I couldn’t see her.
(C. Erickson, personal communication, October 12, 1992.
Sheronda needed a summer school placement for all 3 months, something
that the program she
had been attending did not offer. Consequently, in the summer before her
fifth birthday, she moved to an all-day child care program in a private
Montessori preschool. The same special education supports and services
that were available in the previous school were made available to
Sheronda in this program. Sheronda continued to progress and adjusted
very well to the child-initiated work routine that was part of the
program’s method. It was during this time that she first spoke. Excited
to hear about the details of this important event, we eagerly asked for
the story:
[What did she say? Who did she talk to? What was going on when she
talked?] “Move, please [to a peer who was a little too close to
her materials].” (J. Keating, personal communication, April 10, 1993)
Sheronda’s mother was and remains closely involved with each of
Sheronda’s experiences and
programs. Her mother faithfully attended biweekly and the monthly core
team meetings on her day off from work in order to communicate with
Sheronda’s preschool staff and special education teacher. She visited
the elementary school that Sheronda would attend and met with the
principal and the multi-age classroom teacher in the spring before
Sheronda’s entry into primary education.
Sheronda’s mother is an involved parent in the school. She knows what
she wants for her daughter and is comfortable planning and working with
professionals as an equal member of a team.
Insights from the Stories
Many more stories could be related like these about Dana, Ashley, and
Sheronda, stories that
portray the powerful transformational moment that can occur upon first
seeing a child with significant disabilities within an accepting
inclusive setting. This is a moment when our assumptions about a child
are unexpectedly suspended as we see them through a different frame of
reference. The “Aha!” moment occurs when a shift in paradigms becomes
possible (Covey, 1989, Kuhn, 1970) and one truly understands what it
means to see a child with significant disabilities as a child with the
same rights and needs for a joyful childhood as all children.
These stories offer evidence of what the participating adults have noted
consistently: Young children do not view or respond to the presence of a
person with disability as adults do. The stories offer powerful
confirmation of the belief that early childhood is the most opportune
time to begin breaking down the societal barriers and discrimination
that confront those with disabilities and their families.
Our observations, however, do not suggest that the typically developing
children are unaware of
the differences presented by their friends with significant
disabilities. Their countless questions
related to disabling conditions of their classmates show that hey are
aware. Comments such as these offer evidence of their interest in and
need to understand the differences they recognize in their peers: “I never knew a 5-year-old who couldn’t walk on the bottom of the pool,” “Why can’t he say it with his mouth?” (i.e., talk), and “Why does he
spit all the time?” (i.e., drool) (Thompson, Wickham, & Wegner, 1991).
Children's questions about their classmates with disabilities do not,
however, reflect value judgments about individual worth, signal
rejection, or suggest a questioning of a classmate’s right to be
part of the same setting (Shanks, 1990). It is common to hear a child
repeat the content of an adult’s response to explain something about the
child with a disability to another classroom peer or to a new adult in
the setting. A child may repeat this information even he or she did not
ask the question, but was present and listening when it was first
answered. The role of informant, interpreter, and facilitator for a
child with a disability is often naturally assumed by his or her
typically developing friends who are 3-5 years of age. A child who has
never asked a single question, but who has watched a classmate who
experiences a disability with interest and openness, may offer an
explanation like this:
Jacob can’t talk because his muscles don’t work very well, but he knows
all about the sound cylinders. He can’t shake them ... he nods his
head if they are the same. He knows all about them.
OUR WORK AND OUR VALUES
As noted in the introductory section of this chapter, CIP has been directed toward the inclusion of young children with the most severe disabilities into a variety of early childhood programs that predominantly serve typically developing children. CIP has focused on initiating and implementing inclusive early childhood program services and on investigating and documenting important features of those services. The implementation of inclusive early childhood services has involved 1) starting the process, 2) preparing and then providing ongoing support for families and personnel, 3) accommodating the often intensive and individualized needs of children and families, and 4) providing ongoing facilitation of the social and instructional inclusion of children. This section describes CIP in greater detail.
A Value-Based Approach for Program Strategies
The strategies employed by CIP are grounded on an understanding and application of a milieu and naturalistic approach to meeting the needs of young children by embedding instruction and therapeutic services into existing activities and routines of the natural setting (e.g., home, child care center/preschool) (Bailey & McWilliam, 1990; Bricker & Cripe, 1992; Guess et al., 1978; Kaiser, Hendrickson, & Albert, 1991; Noonan & McCormick, 1993). In addition, attention has been directed to procedures that result in the meaningful inclusion of the children and their families. For example, strategies and variables have been investigated that support sustained positive reciprocal social interactions (friendships) among children and productive relationships among the families and personnel who are brought together within the context of these programs. Early in our work together, a value base was articulated in the form of seven value statements that guided CIP procedures and activities (see Table 1).
|
Table 1: The Circle of Inclusion
Value Statements Value One We reject the notion that children with disabilities must be “fixed” (frequently couched in terms of meeting certain criteria) before they are ready to take their place in families, neighborhoods, and community environments and experience the normal flow of everyday life and friendships available to children without disabilities. Specifically we are concerned that preschool children with severe disabilities and their families have the opportunity for inclusion in high-quality child care and preschool programs within the mainstream of community programs available to typically developing children and their families. Value Two We recognize that typically developing children must have an opportunity to develop relationships with children who experience disabling conditions, including children with the most significant disabilities. We acknowledge the importance of children learning to live in a pluralistic society and to accept individual differences at an early age. We believe that typically developing preschool children are at a critical readiness period for the experience of knowing a child with a disability and that their lives will be enriched by reaching out to friends who experience disabilities. Value Three Value Four Value Five Value Six Value Seven |
Emergence of the Circle of Inclusion Project
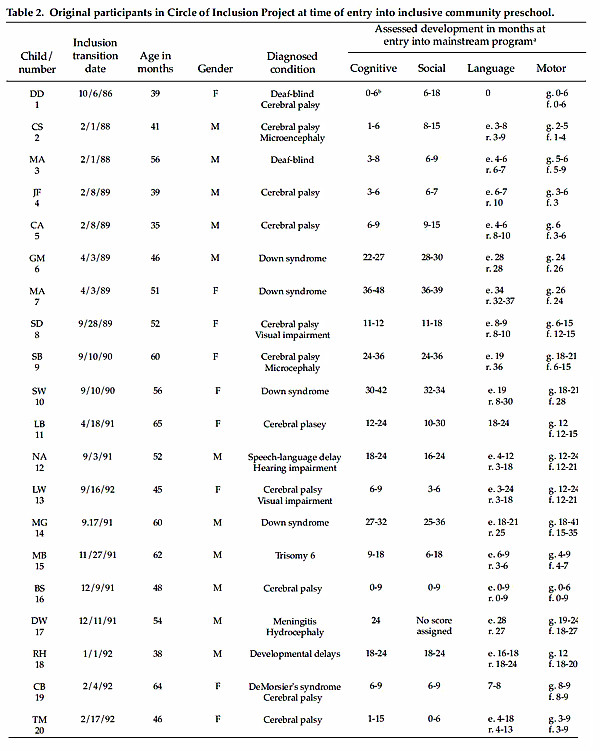
By 1992, 20 children with disabilities, two special education preschools, and four community early childhood programs had participated in CIP. The first 20 children to participate in CIP activities and investigations are described in Table 2, which provides information about these children at the time of their transition into inclusive preschool programs. As can be noted, the children were between the ages of 3 and 5 years, and all had diagnoses, medical conditions, and/or assessed developmental levels indicative of significant disabilities.
What had begun so informally in the fall of 1986 with one child, Dana, was merged into the service delivery systems of two public school districts beginning in the fall of 1992. Two applications were submitted for state grants to support efforts to restructure part of the early childhood service delivery system. Both projects were funded through Title VI-B Special Project state funding from the Kansas State Board of Education to implement programs of inclusive early childhood special education as a service delivery option within the two Kansas districts. The Lawrence, Kansas, project, Project LIM (Lawrence Early Education Program Inclusion Model), and the Kansas City, Kansas, Project WIN) Wyandotte Cooperative Inclusion Network), both focused on continuing to implement and expand components of the CIP.
Recently, CIP components have been implemented,
expanded, and disseminated via two US
Department of Education Office Special Education Outreach Training
Projects. One of the projects
has been directed toward expanding aspects of the model for young
elementary children with severe disabilities and autism, and the other
project has been extended to community training teams to initiate and
implement inclusive early childhood services that address the needs of
children with the most significant disabilities.
The Lawrence, Kansas, model (Project LIM, Lawrence Early Education
Program Inclusion Model) has expanded inclusive services via interagency
agreements with five community early childhood programs and involves
services to children with a full range of delays and disabilities (i.e.,
mild to severe/profound). Approaches to services implemented in this
model include:1) employment of an early childhood special education teacher in two
community preschools that hold openings for placement of children with
disabilities,
2) intensive itinerant early childhood special education services in
Head Start and two additional community preschools that hold openings
for placement of children in the program in which they were enrolled at
the point they are identified for these services.
The Kansas City, Kansas model (Project WIN, Wyandotte Cooperative Inclusion Network) includes children with severe and profound disabilities and children with autism. Children previously served in segregated classrooms in the University of Kansas Medical Center are placed in classrooms with typically developing children that are:
By the end of the school year in 1994, early childhood teachers and
child care professionals in 23
preschool classrooms within 10 community early childhood programs
(including two Head Start
Programs), primary general education teachers in 10 kindergarten
programs, first-grade, and second grade classrooms, as well as personnel
from early childhood special education programs in two communities
(Lawrence and Kansas City) received training to implement inclusive
programs for young children with severe disabilities (Thompson & Wegner,
1993). At that point, more than 600 typically developing children and 35
children with severe disabilities had participated as members of
inclusive classrooms that employed components of the CIP model.
OUR KNOWLEDGE ABOUT KNOWLEDGE: A SUMMARY OF RESULTS AND OUTCOMES
Early in our work together in the implementation of inclusive early
childhood services for preschool-age children with significant
disabilities, we began documenting the experiences and reflections of
all the participants. We kept field notes in which we recorded events
and experiences as they happened, along with notes reflecting our
thoughts and feelings in the role of participant-observers.
We also periodically made audio tapes of interviews with the involved
parents and professional so we could have verbatim transcriptions of
their thoughts and recollections. Extensive videotape records of the
children directly participating in inclusive classes, which now span 10
years, were also maintained and have been a rich source of data as well
as a resource for training. In addition, we conducted a number of
observational studies using internal and time-sampling approaches for
data collection and single-subject experimental studies that validated
and provided insight into what we believed we understood through our
participation.
We became convinced that a combination of qualitative and quantitative
approaches offers a
particularly rich environment for understanding the development and
evaluation of new program models within a system change endeavor. As
already noted, our multifaceted approach has been grounded in
observation, data gathering, reflection, and direct participation over
10 years of creating and maintaining inclusive and family-centered
services. Inherent in such an approach is the flexibility to adjust
perspectives and units of analysis. A qualitative approach made possible
a holistic view of a complex system and offered a means of addressing
multiple components of the program and its impact. Linking a
quantitative approach to this process offered opportunities to verify or
reject impressions and to discover other factors of importance. Three
studies primarily addressed qualitative components of our work (Perez,
1992; Stargardter, 1988; Thompson, Wickham, & Wegner, 1991). Six
studies conducted as part of the project involved direct observation and
coding of environmental, adult, and child variables; and several studies
involved comparing a range of variables such as training
procedures, equipment, adult style, and setting characteristics across
programs, children, and personnel (Brooke, 1992; Kimura, 1991; Lit,
1993; Stegemann, 1993; Wegner, 1991; Wickham, 1993).
We focus on providing an overview of nine themes that emerged as
meaningful for organizing
results from specific studies, informative experiences, and outcomes of
our program (Thompson & Wegner, 1993). The themes discussed in this
chapter include:
While offering
specific findings
and impressions, liberty has been taken to interpret some of the results
and to emphasize important implications.
Factors Affecting Program Success
Acceptance of the inclusion program and its overall success (long-term
participation and quality
implementation) seemed to be highly related to the extent to which both
the director of a community program and the program’s early childhood
teachers held a consistent, articulated philosophy and a sense of
mission centered around meeting the needs of children and families.
Examples of the kinds of programs with which we have worked most
successfully and that operate with an explicit philosophy and sense of
mission are Montessori programs, Head Start programs, and National
Association for the Education of Young Children (NAEYC) accredited
programs. Other features of programs that we generally considered as
having had an impact on success included program longevity and
reputation in the community, employing of qualified teachers, low staff
turnover, and a stable financial base for the program.
The education of children and youth with significant disabilities has a
history of implementing
teacher-directed approaches (Guess & Thompson, 1990; Thompson & Guess,
1989). Despite this fact, we have consistently found that classrooms
with a child-initiated, child-centered to early childhood education
grounded in developmentally appropriate practice (Bredekamp, 1991) seem
particularly able to sustain the successful placement of young children
with significant disabilities.
We have had long-term, successful experiences with the Montessori
approach to early childhood
education (Thompson, Wickham, Ault, et. al., 1991). For example, the
initial placement site for our program, a private Montessori program
accredited by the American Montessori Society, has increased its
involvement over the past 10 years. One of the teachers was appointed as
the coordinator for special education services to ensure optimal ongoing
placement and coordination with the public school early childhood
special education certification with a specialization in children with
severe disabilities. By 1992, part of her salary was paid through a
contract between the public schools and the private community program.
Another teacher in the same program has begun graduate work in special
education, and two additional teachers have worked actively with the
multidisciplinary teams who serve children in their classrooms. This
program also added ramps, purchased adaptive equipment (such as a
toilet), installed a visual fire alarm, and altered the playground to
increase accessibility.
A number of considerations make Montessori programs an attractive model
for the inclusion of
young children with significant disabilities (Thompson, Wickham, Ault,
et. al., 1991). Certified
Montessori teachers must meet rigorous performance standards and are
well-qualified early childhood educators. In addition, Montessori
environments have features associated with developmentally appropriate
practice as articulated by NAEYC guidelines (Bredekamp, 1991). These
features include mixed age groups, child-initiated focus of the
classroom with a predictable structure, prepared classroom environments
that enhance choice and autonomy, and a rich array of functional and
interesting materials that can meet a wide range of developmental needs.
A practical consideration relates to the relative consistency in the
curriculum and method of replicating effective procedures across
multiple settings. (For other relevant features of the Montessori
approach, see Chattin-McNichols, 1992; Krogh, 1982; Lillard, 19973;
Loeffler, 1992; Safford, 1989; Thompson, Wickham, Ault, et. al., 1991;
and Wegner, 1989.)
More recently, Head Start programs have become actively involved in the
inclusion efforts of both districts we worked in, and eight Head Start
classrooms in two communities have participated in our program quite
successfully. The relationship with Head Start was facilitated by the
Head Start regulations, which support collaborative arrangements with
school districts and call for the inclusion of children with severe
disabilities (Division for Early Childhood of the Council for
Exceptional children, 1993). Although Head Start classrooms may
implement a variety of curriculums, two approaches that are frequently
implemented and are particularly viable for inclusion include the High
Scope program (Hohmann & Wiekert, 1995) and Creative Curriculum (Didge &
Colker, 1992). Several noteworthy features of Head Start include the
high level of involvement with families, the broad range of health and
nutritional programs available to children and families, and ongoing
required staff development activities.
It should be noted that the child care components of the inclusive
community programs were
consistently used by families and were often the reason they preferred
one community program over another (Thompson & Wegner, 1993). As
conveyed in the literature (Berk & Mense, 1990) and reflected in our
experience, finding child care for children with significant
disabilities is very difficult for families. By starting relationships
with programs for inclusive early childhood education, doors were opened
to many children for extended child care.
Finally, the issues of accessibility of a program for children with
significant physical challenges
has definitely been a factor in whether a program worked or not. While
making shift, temporary
adaptations are often possible, some programs are located in buildings
in which it is virtually impossible to safely include a child with
significant physical challenges. This fact has important implications
because accessibility has an impact on the safety of all young children.
Evidence of Participation of Children and Partners
Although we have documented countless touching personal observations of growing relationships among children with significant disabilities and their typically developing peers, we have also documented quantitative evidence of the children's experience. During a period of split enrollment in both an inclusive preschool and a special education preschool, three studies documented and compared aspects of the same children's communication, engagement in activities, and interaction with partners in both settings (Brooke, 1992; Stegemann, 1993; Wegner, 1991). The Brooke and Stegemann students used the CEVIT (Coding Environmental Variables and Interaction on tape) (Kimura, 1991; Leon, 1992) to code interactions and environmental variables of the same three children in the two settings. Each student sampled different episodes during a similar time period. The Stegemann (1993) study used exactly the same video episodes as the Wegner (1991) study. The observational analysis conducted by Wegner involved the analysis of verbatim transcripts obtained from the video episodes. All three studies involved comparisons of data for statistical significance. The results indicated that an inclusive setting offers more desirable social and communicative environment for children with significant disabilities on both a quantitative and qualitative basis and that it matches a high-quality special education program on environmental adaptations. Some of the most interesting conclusions derived from these studies are summarized here:
Children with severe disabilities had significantly more peer partners and more communicative interactions in the inclusive community preschool than in a special education preschool.
The children initiated more frequently and took more participatory turns in the inclusive community preschool
The children interacted with more children in the inclusive community preschool than in the special education preschool.
The children interacted with more adults in the special education preschool than in the inclusive community preschool.
The length of time a child with a severe disability engaged in a single activity was consistently longer in the community preschool than in the special education class, although the difference was not significant. Furthermore, children with disabilities tended to spend more time on activities within a mainstream program over time.
Accommodations (e.g., adaptive equipment for supporting positions, augmentative communication devices, and provision's for accessibility of materials) in an inclusive program were comparable with those provided in high-quality special education classrooms. In addition, children with significant disabilities spent more time out of their wheelchairs and engaged in floor and table activities in the inclusive program.
When compared with adult partners in a special education program, adult partners in the inclusive community program were more facilitative of communication in their interactions with children with severe disabilities. Adults invited response, offered choice, redirected others to interact with the child, and interpreted the child's nonverbal responses as communicative significantly more often than did the partners in a special education program.
When compared with adult partners in an inclusive program, adult partners in a special education program were more directive in their interactions with children with severe disabilities. They gave commands and instructions significantly more than did the children's partners in a mainstream program.
Peer partners in the inclusive community preschool initiated more frequently, took more turns, and used more redirections than did the peer partners in the special education preschool.
Influence of Adults on the Development of Friendships Among Children
The results of this project confirmed the importance of the role of the adult partner in the development and maintenance of peer interactions among children with significant disabilities and typically developing children (Brooke, 1992; Lit, 1993; Stegemann, 1993; Wegner, 1991; Wickham, 1993). Frequently, adults must mediate initial peer interactions by offering support for interaction. Successful strategies included:
Children with significant disabilities do form special relationships
(friendships) with some of their
typical peers that appear to be mutually satisfying and are maintained
when the children are in the classroom together. Evidence of such
friendships includes reports of the typically developing
children's comments to their parents (Perez, 1992), invitations to play
or attend parties (Stargardter, 1988; Thompson, Wickham, & Wegner,
1991), and consistent interactions over time among the children as noted
in observational records and videotaped episodes that show the presence
of peers (Brooke, 1992; Jenson, 1994; Kimura, 1991; Leon, 1993; Shanks,
1990; Stegemann, 1993; Wegner, 1991).
Some of our conclusions and observations related to the process include
the following:
Preparation for first meeting the child with a significant disability, although often part of inclusion programs for school-age children, need not be extensive with very young children because their attitudes are still being formed rather than changed; and information is sought quite naturally (Shanks, 1990; Thompson et al., 1991).
Although children are apt initially to place a child with severe multiple disabilities on a parallel with infants and toddlers, this view diminishes over time as information about the child and his or her disabling condition is offered typical peers (Shanks, 1990; Stargardter, 1988; Thompson et. al., 1991).
Children with typical development or with mild disabilities follow the model of adults in communicating with children with significant disabilities. If adults are facilitative partners, the children are more facilitative partners; if adults are directive partners, the children are more directive and more likely to refrain from involvement in cooperative activities with a child who has significant disabilities (Lit, 1993; Wegner, 1991).
Same-age peers who are friends with children with significant disabilities learned to use supportive strategies that are related to physical assistance and facilitative support (e.g., supporting a friend's head and arm, supporting a friend's trunk, wiping saliva from a friend's chin, providing with assistance to eat, pushing a wheelchair, getting necessary positioning materials, presenting and handling materials, interpreting communications, selecting activities that their friend previously enjoyed) (Jenson, 1994; Lit, 1993; Stegemann, 1993; Wegner, 1991).
Children responded fearfully to a child who was aggressive to them and noticed asocial and unusual behavior (e.g., stereotypy) (Thompson et. al., 1993). They also accepted explanations of the communicative and/or coping nature of such behavior and the need for their peer to acquire new strategies. Typically developing children persisted in interactions with children whom they initially feared or avoided and assisted their classmate in practicing new strategies, generally but not always with adult support and encouragement.
Accommodations for Welcoming Environments
Environmental accommodations should be planned through ongoing
environmental assessment,
and the initial lack of adaptation should not be used as a reason to
reject placement in an inclusive program.
Our review of videotapes and direct observation consistently indicated
that there was more focus in the inclusive settings on how
accommodations would enhance participation than in the special education
settings (Brooke, 1992; Stegemann, 1993; Wegner, 1991).
When children required specialized equipment and devices, many early
childhood teachers found it helpful to explain and demonstrate equipment
and devices as part of a large group activity in which its purpose and
use were presented in a manner that was respectful to the child who
would be using it and, to the extent possible, involved this child's
position and keeping the child with a disability on a face-to-face level
with his or her peers was important (Thompson et. al., 1993).
The availability of ongoing support for assistive
technology was used. Much time and considerable difficulty were involved
in identifying appropriate assistive technology devices such as
augmentative communication devices, as well as in programming the
devices, identifying appropriate and functional child positions to
facilitate effective use of the devices, and teaching children and staff
to use the devices correctly (Thompson et. al., 1993). The factors that
interfered significantly with the availability and use of augmentative
devices in an inclusive setting seemed very similar to the problems
associated with these devices in self-contained special education
programs.
Finally, the use of specific equipment does not appear to negatively
affect interactions among
children. In fact, using a device such as an augmentative communication
device in an inclusive
program offers many more opportunities for practice in using the device
with speaking partners who are also peers in natural situations.
Further, devices and special equipment often served as attractors for
partners who were curious about them and interested in using them. In
fact, one might venture to say that these devices sometimes took on a “status” quality. Pushing a child in a wheelchair was a highly valued
activity. One 5-year-old who was negotiating with her classmates for how
they might merit invitations to her birthday party was overheard
approaching Shannon, who had just received a communication device. The
child told Shannon that she could be one of the lucky invitees if she
would “bring her box” to the party (D. Leon, personal communication,
April 16, 1991).
Experiences and Perspectives of Parents of Children with
Disabilities
Our experiences over 10 years offered us some important insights into
the experiences of parents. The concerns and fears expressed by
parents of children with disabilities and personnel before transition
into inclusive environments are consistent with a body of emergent
literature (Hanline, 1993).
Over the course of this project, we experienced a shift in parents' awareness of inclusion. Initially we had to invite parents to consider
participating, whereas parents are now requesting, and sometimes,
insisting on, inclusive placements. Following are conclusions about the
experiences and perspectives of parents and about strategies that were
successfully implemented to facilitate the process of inclusion for the
family (Thompson et. al., 1993):
Parents who had experience with special education preschool programs with high staff-to-child ratios sometimes expressed concern over their lack of contact with the regular education teacher.
Some parents were less likely to attend general early education conferences and programs offered by the inclusive community program than those offered by the explicitly special education components of the program. Formal ways of linking these families with families of typically developing children who are in the program were needed to enhance the feeling of belonging for parents of children with severe disabilities.
The parents and personnel tended to become more positive about the effects of inclusion on the children after direct participation in a program.
Participation in an inclusive early childhood program appeared to affect the parent’s placement preferences for inclusive school-age services. This result had an impact on the transition to school-age services (kindergarten and primary grades in elementary schools) and will ultimately have an impact on the nature of special education services through the life span.
Whether or not parents requested the placement, activities, and strategies for involving and informing parents were critical (e.g., tours of program, involvement in environmental assessment, small group meetings with veteran parents, a handbook). The MAPS, Making Action Plans or the McGill Action Planning System (Vandercook, York, & Forest, 1989), which is based on a futures planning approach that has been adapted for educational planning, was also useful for initiating the child's entry into a program and developing an individualized education program (IEP).
A way of ensuring ongoing and frequent communication was very important. Daily notebooks were particularly useful for some families. The parent, early childhood teacher, and special education support team members all communicated in writing through the use of notebooks.
Parents who participated as members of a core team that met bi-weekly or monthly to problem-solve and plan participatory strategies for the child in the classroom seemed most involved and empowered.
Parents of children in an urban setting tended to demonstrate less confidence in advocating for their child with public school personnel. However, their interest in inclusive experiences and their need for child care were similar to that of the parents in more affluent, suburban communities.
Experiences and Perspectives of Parents of Typically Developing Children
Parents of typically developing children can be valuable resources. Although we did not sufficiently explore strategies for involving these parents, results suggested that parents of typically developing children should be educated and involved along with parents of children with disabilities and participating personnel. The following points all emerged from Perez’s (1992) qualitative study of eight parents whose typically developing children had formed special relationships with their classmates who experienced significant disabilities:
Parents of typically developing children supported the concept of integration at the preschool level and recognized that integration can be beneficial for their typically developing children, as well as for the children with disabilities. More specifically, parents stated that exposure to people with disabilities fostered acceptance and contributed to important changes in society.
Without prompting by the interviewer and without responding to a specific question, all parents we formally interviewed brought up the role of the additional paraprofessional as an integration facilitator in the classroom. All these parents indicated that the addition of a knowledgeable person who could assist the teacher and the child with a disability was the most important factor in making the program work.
Most parents indicated that while their children expressed acceptance and positive regard for their peers with disabilities, their children did not talk much about their peers with disabilities at home or describe any special type of relationship with them. Parents said that their children talked about the children in the school, although parents were also quite sure that their children were aware of the peers' disabilities. One parent noted that her little girl sometimes played “handicapped preschool” with her dolls.
Conversely, the parents of a 5-year-old boy talked about the lengthy and detailed comments of their son about his friends with disabilities. This was consistent across 3 years of preschool. His parents attributed his close attachment to his friends with disabilities (three different children over a 3-year period) as instrumental to his adjustment and happiness in the program. Interestingly, these were also parents who expressed initial concern that the presence of children with disabilities would take too much teacher time away from their son.
All of the parents indicated that they lacked specific knowledge about integration programs, but although they would like to know more about the program in which their child participated, this lack of information did not affect their positive attitude toward the concept of inclusion.
In general, parents of typically developing children were open to and supportive of the inclusion of children with severe disabilities under the circumstances of CIP, in which the number of children with disabilities in a single classroom generally reflected the natural proportions in the population at large. Although parents did not use the term “natural proportions,” they were clearly aware of this issue and spoke about ratios of children with typical development and children with disabilities.
Transitioning for Adults to Inclusive Services for Children
The immense power of the involved personnel to affect program success or
failure must be recognized, and the need to educate and support
these adults cannot be overemphasized. Although special education
personnel working with children in inclusive settings initially
expressed concern about their roles, most believed it was their
responsibility to give their best effort for the sake of the children
and were willing to sustain a period of discomfort to that end
(Stargardter, 1988; Thompson, Wegner, et. al., 1991). Conversely, the
general early childhood staff indicated pleasure at the opportunity to
participate in an inclusive program, but expressed concern about their
ability to meet the needs of the child and about the degree of support
and assistance they would receive. Fear of actually handling a child
occurred consistently as a new program began including a child with
significant disabilities.
As relationships with other professionals and families developed around
addressing the needs of
a child, most special education personnel became more positive and
supportive of inclusive practices; and most general early childhood
personnel became more comfortable and more interactive with the
children. However, the search for strategies that fit this new paradigm
from both special and general early childhood personnel seemed ongoing.
Over 10 years we have encountered a number of issues related to the
involved personnel and their work that discuss the following topics
including:
When two or more service delivery models exist within a community, competition may occur between the two program staffs. For example, when the split program arrangement was used (children attended a special education classroom for half a day and a community preschool for the remaining half day), issues arose over which program was benefiting the child the most, although some professionals described this split as the best of both worlds (Stargardter, 1988).
This underlying sense of competition also arose when one component of a school district early childhood special education program moved to an inclusive model and another component of the same program did not.
Role confusion and frustration are major factors
that can negatively affect the satisfaction of all
personnel. The need to invent some strategies to match the needs of a
new program model was
particularly disconcerting to some personnel. As the number of community
programs increased, the need to tailor one’s role to best fit the
specific staff and children within the programs, each of which
functioned quite differently, placed great demands on personnel to be
flexible and inventive. For example, the way that many of the related
service professionals scheduled their time did not really fit the needs
of some programs and children. In some cases, scheduling related service
professionals with children in an inclusive program for a less frequent
and shorter periods, was found to be more productive for effective
consultation, transdisciplinary training, and integrated therapy (e.g.,
an occupational therapist spending all morning with a child in a
preschool program every 2 weeks instead of two or three 20- to 30-minute
sessions per week).
In-service training related to teaming, collaboration, and problem solving was valued and constantly sought by participating personnel. In retrospect, we believe we should have included more content related to understanding personality types and differing work styles as useful information for anticipating the reactions of some personnel to functioning in a program that requires inventiveness.
A more thorough grounding in the process of system change would also have been desirable to assist individuals in anticipating their experiences and reactions.
One of the most common sources of confusion seemed to stem from a lack of understanding and respect for other program and personnel practices. Special education and related service staff needed to be informed about early childhood program models and procedures. Frequently these individuals did not have a background in early childhood education and in some cases lacked knowledge of child development. Personnel who were accustomed to working only with children with very significant disabilities within a segregated program setting sometimes had difficulty entering an inclusive environment in a productive and respectful way.
As investigators with long histories of working in segregated special education settings, we were aware of the tendency for adults to talk to adults in a classroom in which none of the children are able to speak. One scenario with which we are all familiar is a special education teacher or therapist showing another adult how to work with a child and offering a clinical explanation of a procedure in the presence of everyone (children and adults) in the classroom. This was often viewed by the early childhood program staff as demeaning to the child, a way of negatively setting the child apart from his peers, and as rude and disruptive. (Need we mention professionals walking into a classroom with a coffee cup and engaging in personal conversations?) Another scenario with which we are also familiar is the self-contained preschool program for children with significant disabilities in which there are as many (or more) adults as children present. We found it necessary to give considerable attention to minimizing the intrusion of specialized staff serving a child in an inclusive program.
Of course, early childhood educators and child care workers need to learn about the roles and contributions that related service personnel and special educators can make. They too must learn to adjust to becoming part of a team, opening their classroom to the expertise of other professionals and their suggestions about working with a child with significant disabilities. This collaborative attitude was hampered or enhanced to the degree that the early childhood program staff felt empowered as principal players on the team, valued rather than judged, and supported rather than intruded upon.
Paraprofessionals as Facilitators
The adult-child ratios for children in most early childhood programs (1 adult to 10-12 children) must be enhanced if a child with significant disabilities is to be included. Attention to the training of all classroom personnel and the investigation of a range of approaches for increasing adult support are still needed. One of the approaches used in CIP was to assign an additional assistant to the inclusive community classroom and to have the school district pay this person as a paraprofessional. This individual functioned in a variety of ways and was generally co-supervised by the district early childhood special education teacher assigned to work with the children and personnel in the community program and by the early childhood teacher in charge of the classroom. In some cases, this person functioned primarily as a classroom assistant across children and tasks. In many cases, however, this person functioned as a “facilitator” for the child with significant disabilities. This was most true when a child had significant and multiple physical and sensory challenges that limited the ability to move or participate in an activity.
The explicit assigning of a paraprofessional to a specific child in an inclusive preschool had both advantages and disadvantages, and these issues have been raised by a number of individuals involved in inclusive programs (Giangreco & Putnam, 1991; York, Vandercook, Caughey, & Helse-Neff, 1988). The results of several studies indicated that an individual serving as an “integration facilitator” of an adult partner was beneficial to a child's communicative competence, as well as supportive of the child's meaningful participation in the settings (Stegemann, 1993; Wegner, 1991; Wickham, 1993). The strength of this approach included the presence of someone who was able to become extremely sensitive and “tuned in” to a child's nonverbal communication, thereby empowering the child to be heard and to be a more active communicator and social participant in the classroom. The facilitator’s role could be compared with the role of an interpreter. In addition, the individual taking the role of the facilitator became very skillful in supporting a child's ongoing physical participation, which is critical for a child with extremely limited movement capabilities.
Adults with good skills in relating to young children attracted more partners for a child with significant disabilities (Lit, 1993), while still providing the intensity of support and instruction required by children with significant disabilities. As noted earlier, adults are initially the primary interpreter and are usually essential in facilitating new relationships between children. There remains, however, a significant need for more research about how adults can recognize when child-to-child interactions can be maintained without their support and how to fade from these interactions.
We also found problems associated with the assigning of a paraprofessional to a particular child. Our data indicated that paraprofessionals supporting the inclusion of children with disabilities sometimes appeared to negatively affect the frequency with which the regular early childhood teacher interacted with the child (Lit, 1993). It was fairly common for a facilitator to become overly attached to a child and to prevent the rest of the classroom staff from becoming meaningfully involved with the child. Another problem that sometimes arose was the tendency for some early childhood classroom teachers to turn over complete responsibility for the child to the paraprofessional facilitator.
This result brought the loss of an appropriate teacher-child relationship and inhibited the child's true membership in the class group.
Preparation of Adults to Serve as Child's Partner
Individuals supporting the inclusion of a child are likely to miss opportunities to support interactions, instruction, and participation unless directly trained to do so (Wickham, 1993).
Instruction on facilitative strategies that support child-to-child interactions for all adults who were involved with the program was necessary to ensure application of these strategies in the classroom. Direct training using videotaped episodes of children and paraprofessionals in inclusive classrooms that were part of CIP was conducted by Wickham (1993). The results of this study indicated that this training was an effective way to enhance the use of strategies that facilitate child-to-child interactions and specialized instructional procedures. Paraprofessionals in training viewed video taped episodes of their interactions within a classroom, focused on observing specific strategies, and reflected on possible improvements with a specific trainer. Their results were moderately encouraging in regard to generalization to other children and maintenance over time, but suggested that ongoing and direct training is important for a considerable length of time.
FINAL COMMENTS AND RECOMMENDATIONS: FEATURES OF AN EXEMPLARY PROGRAM
Our prolonged involvement with CIP has contributed much to perspective on the short- and long-term issues regarding inclusive services for young children with significant disabilities and the sustain ability of emerging programs. Mindful that approaches to the development of service models should meet standards of exemplary practice, as well as reflect the unique characteristics of the community in which they are implemented, we have developed recommendations for features of an exemplary program (Thompson et. al., 1993). These recommendations are designed to enable programs and personnel to move from the “believing” to the “doing” stage and to establish a lasting structure.
Embracing a Shared Value Base and Vision
The establishment of a set of values (see Table 1) to which a very diverse group of individuals ascribed made it possible to transcend a number of the differences in agency functions and procedures as well as in participating program approaches to early childhood education. These shared values and the vision of inclusive early childhood education and child care for all young children and their families provided the impetus to continue the program over a number of years.
Participation of Community-Based Early Childhood Programs
A broad number of “community-based programs” including private for-profit, private not-for-profit, and head Start programs that predominantly serve typically developing children offer potentially excellent programs for the inclusion of young children with significant disabilities.
One of the most compelling rationales for involving community programs is the opportunity for families to have the same options for selecting programs as do families of young children with typical development. Parents may have preferences based on a particular community program or may have attended a program with which the parents are comfortable.
Using Varied Approaches to Provide Inclusive Classrooms
A number of approaches offer communities ways to move toward
establishing inclusive services
for young children. These approaches include: 1) contractual
arrangements that support certified
staff who are employees of the community programs; 2) blended
classrooms, such as the emergent practice of blending Head Start and
early childhood special education programs or arranging for team
teaching between an early childhood special education teacher takes on
an itinerant role and works with staff and children in several programs.
In some communities, two or more of these models are used in combination
as they were in the programs employing components of CIP.
Creative and Flexible funding via Interagency Relationships
Sources of cost that are likely to be specifically associated with an early childhood inclusion program for young children with significant disabilities include child tuition and fees, additional personnel, facility accessibility adaptations, licensing adaptations, special equipment and materials, staff education programs, and numerous family programs. Administrative personnel involved in an early childhood inclusion program must have a good understanding of the potential resources available to the various agencies and individuals who might participate in the program. When several agencies work together (e.g., school district, head Start, community preschool, and child care centers), a creative and resourceful funding base can be built to support the program model that meets the unique needs of the community and is also responsive to the individual needs of families.
Linkage with Programs Offering Child Care Services
One solution to the problem of limited or nonexistent child care options for young children with significant disabilities is to assist service providers in existing child care programs to accept youngsters with severe disabilities and to assist families in gaining access to these services. A particularly viable application of this solution is to offer inclusive early childhood services in programs that offer full-day child care.
Providing High-Quality, Child-Centered Programs with Developmentally Appropriate Practices
As Safford (1989) points out, there is inherent value in good early childhood practices for all children; and considerable benefit can derive from using child-specific adaptations and interventions with teaching approaches appropriate to all children. Characteristics of child-oriented programs that support active learning include:
Facilitating Membership Through Supported Placement
The use of a paraprofessional or another adult assigned as a classroom facilitator for a child with significant disabilities can offer the intensive support needed by children with severe disabilities within inclusive programs. In our experience, the inclusion facilitator plays a pivotal role in how well a child is accepted into a classroom because the facilitator often determines whether interactions occur or do not occur with other children and program staff. Interactions with young children with severe disabilities are fostered by teaching children to act as responsive and sensitive partners, by providing opportunities for meaningful interactions with peers, and by supporting a child in an interaction if he or she needs support. The person working directly with a child with a disability in an inclusive early childhood classroom must be a careful observer of children's behavior and must be sensitive to communicative attempts in order to promote interactions between children that are sustained, but not continuously supported by an adult. Using strategies that facilitate interactions among typically developing young children and their classmates with disabilities allows children to determine the content and direction of their interactions, encourages true communication, and fosters an environment in which friendships can unfold.
Establishing Collaborative Teams Based on Functional Tasks
Effective team functioning requires that all team members, including
parents, share a common
philosophy and commitment to the development of the whole child and be
able to communicate
openly and effectively with one another (Rainforth, York, & Macdonald,
1992; Swan & Morgan, 1993).
An inclusive program model compounds the already complicated process of
teaming because members often represent multiple community agencies,
each with different administrative patterns, missions, and philosophies.
Furthermore, the complex and intensive needs of children with
significant disabilities and their families require an intensive effort
on the part of the child and family team.
Joint Service Provider and Family Preparation
Staff and family preparation activities are absolutely critical to ensuring that each individual optimally approaches the shift to inclusive services (Klein & Sheehan, 1987). Participants must become acquainted with the nature of systematic change and the need to be proactive and inventive. The role confusion and negativity often experienced in a new program can be reduced by providing opportunities for participants to communicate wit other members of the team about issues affecting their roles and by empowering participants with opportunities to affect their own role.
It is also essential that involved service providers show respect for individuals from programs and agencies that operate under different regulations and use different methods. Participants must learn how to enter a new system by suspending their assumptions about how things should be and follow the advice offered by Stephen Covey in his discussion of the habits of highly effective people: “Seek first to understand and then to be understood,” and “Diagnose before you prescribe" (Covey, 1989).
Service providers must learn this approach to work independently, with each other, and with families from diverse backgrounds and cultures. Ultimately, if we want individuals to work together in a collaborative and open manner, it is essential that we offer joint not separate, education and development activities.
Family-Guided Decision Making and Family-Centered Services
A consistent frustration faced by families as they seek to establish exemplary services for their child and to maintain these services throughout the life span are the lack of a truly seamless service system, and professional resistance to empowering families and to the assertive stance taken by many families. Although family involvement is a principle espoused with the best of intentions by all early childhood interventionists (Bricker, 1989; Peterson, 1987; Raver, 1991), the processes and procedures that include the family in meaningful self-determined activities are still sorely lacking (Bailey & Wolery, 1989; Bricker, 1989; Whitehead, Deiner, & Toccafonndi, 1990). Our experiences with the CIP project confirmed this reality. Changing the way professionals interact with parents continues to be one of our greatest challenges. Program procedures must be implemented that offer promise for empowering families and help service providers value the interdependent nature of their work with families.
SUMMARY
It seems fitting to conclude this chapter with one of our favorite anecdotes, not only because it is humorous, but also because an important concept is voiced so clearly by the words of a child: Five-year-old Shannon, a charmer with big brown eyes and a ready smile, experiences multiple disabilities. Shannon has a condition of microcephaly and cerebral palsy that is predominant on her left side. She is ambulatory, but non-oral. She also experiences intensive grand mal seizures which required that the community pre-school have an emergency medical plan in place and included the immediate notification of an EMT unit. Finally, Shannon's condition is related to prenatal exposure to the cytomegalovirus (CMV). Although medical testing revealed that she was not currently shedding the virus, the community preschool personnel needed to take precautions related to infection control and limiting contact with pregnant staff and parents.
During the production phase of a video tape about the program of inclusion for young children with severe disabilities, four-year-old Sophie, also a charmer with blonde hair and blue eyes, was asked to comment about her classmate Shannon. One of the production crew members who was curious about what the children with typical development thought about the inclusion program was overheard asking, “Well, Sophie, do you think Shannon should be at Raintree or maybe do you think she should go to a preschool for other children just like her?” Sophie, after a short and what seemed as a reflective pause, responded. “No, she should go to Raintree, because – because, how would all the children know who the teacher was talking to – with everybody named Shannon in that school?” (Thompson et. al., 1993, p. 25).
REFERENCES
Bailey. D.B., & McWilliam, R.A. (1990). Normalizing early intervention. Topics in Early Childhood Special Education, 10(2), 33-47.
Bailey. D.B., & Wolery, M. (1989). Assessing infants and preschoolers with handicaps. Columbus, OH: Merrill.
Berk, H.J., & Berk, M.L. (1982). A survey of day care centers and their services for handicapped children. Child Care Quarterly, 11(3), 211-214.
Bredekamp, S. (1991). Developmentally appropriate practice in early childhood programs serving children from birth through age 8 (expanded). Washington, DC: National Association for the Education of Young Children.
Bricker. D., & Cripe, J.J.W. (1992). An activity-based approach to early intervention. Baltimore: Paul H. Brookes Publishing Co.
Bricker, D.D. (1989). Early intervention for at-risk and handicapped infants, toddlers, and preschool children (2nd ed.). Palo Alto, CA: VORT Corp.
Bristol, M.M. Reichle, N.C., & Thomas, D.D. (1987). Changing demographics of the American family: Implications for single parent families of young handicapped children. Journal of the Division for Early Childhood, 2(1), 56-69.
Brooke, T. (1992). A comparison of an integrated setting versus a special education setting using the CEVIT (coding environmental variables and interactions on tape). Unpublished master’s thesis, University of Kansas, Lawrence.
Chattin-McNichols, 1. (1992). The Montessori controversy. Albany, NY: Delmar Publishers.
Covey. S. (1989). The seven habits of highly effective people. New York: Simon and Schuster.
Day. B.. & Drake, K.N. (1986). Developments in experimental programs: The key to quality education and care of young children. Educational Leadership, 44(3), 24-27.
Division for Early Childhood of the Council for Exceptional Children. (1993}. New opportunities for collaboration: A policy and implementation resource and training manual for the Head Start regulations for children with disabilities. Reston, VA: Author.
Dodge, D., & Colker, L. (1992). The creative curriculum for early childhood (3rd ed.). Washington, DC: Teaching Strategies, Inc.
Giangreco, M.F., & Putnam, J.W. (1991). Supporting the education of students with severe disabilities in regular education environments. In L.H. Meyer, CA. Peck. & L. Brown (Eds.), Critical issues in the lives of people with severe disabilities (pp. 245-270). Baltimore: Paul H. Brookes Publishing Co.
Guess, D., Homer, R.D., Utley, B., Holvoet, J., Maxon, D., Tucker, D., & Warren, S. (1978). A functional curriculum sequencing model for teaching the severely handicapped. American Association for the Education of the Severely and Profundly Handicapped Review, 3, 202-215.
Hanline, M.F. (1993). Facilitating integrated preschool service delivery transitions for children, families, and professionals. In C.A. Peck, S.L. Odom, & D.D. Bricker (Eds.), Integrating young children with disabilities into community programs: Ecological perspectives on research and implementation (pp. 133-146). Baltimore: Paul H. Brookes publishing Co.
Hohmann, M., & Weikert, D.E (1994). Active learning practices for preschool and child care programs: Educating young children. Ypsilanti, MI: High/Scope Press.
Jenson, R. (1994}. Video-based media as a method of illustrating child engagement. Unpublished master’s thesis, University of Kansas, Lawrence.
Kaiser, A., Hendrickson, J., & Albert, C. (1991). Milleau language teaching: A second look. In R. Gable (Ed.), Advances in mental retardation and developmental disabilities (Vol. IV, pp. 63-92). London: Jessica Kingsley Publishers.
Kimura, L. (1991). Reliability anallysis for environmental variables of the CEVIT (coding environmental variables and interactions on tape): A tool for observing young children with severe multiple disabilities in an integrated Montessori school. Unpublished master’s thesis, University of Kansas, Lawrence.
Klein, N., & Sheenanm R. (1987). Staff development: A key issue in meeting the needs of young handicapped chlldren in day care settings. Topics in Early Chidhood Special Education, 7(1), 13-27.
Krogh, S.L. (1982). Affective and social development: Some ideas from Montessori’s prepared environment. Topics in Early Childhood Special Education, 2(1), 55-62.
Kuhn, T.S. (1970). The structure of scientific revolutions (2nd ed.). Chicago: University of Chicago Press.
Leon, D. (1992). Reliability analysis for interaction variables of the CEVIT: (coding environmental variables and interactions on tape): A tool for observing young children with severe multiple disabilities in an integrated Montessori school. Unpublished master’s thesis, University of Kansas, Lawrence.
Lillard, P.P. (1973). Montessori: A modern approach. New York: Schocken Books.
Lit, T.L. (1993). A comparison of integration facilitators of young children with severe disabilities in an inclusive preschool setting. Unpublished master’s thesis, University of Kansas, Lawrence.
Loefiler, M. (Ed.). (1992). Montessori in contemporary American culture. Portsmouth, NH: Heineemann Educational Books, Inc.
Mense, J. (1990). Service assessment of child care and preschool program availability for children with special needs: A descriptive analysis of a Kansas statewide survey. Unpublished master’s thesis, University of Kansas, Lawrence.
Noonan, M.J., & McCormick, L. (1993). Early intervention in natural environments: Methods and procedures. Pacific Grove, CA: Brooks/Cole publishing.
Perez, M. (1992). Parental attitudes and perceptions about integating children with disabilities. Unpublished master’s thesis, University of Kansas, Lawrence.
Peterson, N.L. (1987). Early intervention for handicapped and at-risk children: An introduction to early-childhood special education. Denver: Love Publishing.
Rainforth, B., York, J., & Macdonald, C. (1992).
Collaborative teams for students
with severe disabilities: Integrating therapy and educational services.
Baltimore: Paul H. Brookes Publishing Co.
Raver, S.A. (1991). Strategies for teaching at-risk and handicapped infants and toddlers: A transdisciplinary approach. New York: Merrill.
Safford, P.L. (1989). Integrated teaching in early childhood: Starting in the mainstream. White Plains, NY: Longman, Inc.
Shanks, P. (1990). Rediscovering the potential in a children's house: A handbook for persons facilitating the integration of young children with severe disabilities in a Montessori environment. Unpublished master’s thesis, University of Kansas, Lawrence.
Stargardter, S. (1988). Staff and parents perceptions about the integration of children with severe and multiple disabilities into a community preschool program. Unpublished master’s thesis, University of Kansas, Lawrence.
Stegemann, A. (1993). A re-analysis of videotaped segments of three young children with severe disabilities in two preschool environments. Unpublished master’s thesis, University of Kansas, Lawrence.
Swan, W.W., & Morgan, J.L. (1993). Collaborating for comprehensive services for young children and their families: The local interagency coordinating council. Baltimore: Paul H. Brookes Publishing Co.
Thompson, B. (1994, October). Inclusive programs for young children with significant disabilities: Reflections. Paper presented at the annual meeting of the Kansas Association for the Education of Young Children, Manhattan, KS.
Thompson, B., & Guess, D. (1989). Students with the most profound multiply handicapping conditions: Teacher perceptions. In F. Brown & D. Lehr (Eds.), Persons with profound disabilities: Issues and practices (pp. 3-43). Baltimore: Paul H. Brookes Publishing Co.
Thompson, B., & Wegner, J. (1993, December). Project 2.2: Transitioning young children with severe disabilities from a special education program into inclusive community preschool and child care centers. In M. Rice & M. O“Brien (Co-Principal Investigators), Kansas Early Childhood Research Institute on Transition, Final Report (pp. 1-77). Washington, DC: U.S. Department of Education, Office of Special Education Programs.
Thompson, B., Wegner, J., Wickham, D., Shanks, P., Reinertson, B., & Ault, M. (1991). An investigation of the transition and integration of preschoolers with severe and profound multiple disabilities into a Montessori community preschool program: Program history, features, and research activities in progress, Circle of Inclusion Project. Kansas Early Childhood Research Institute on Transition, Project 2.2. Working Paper No. 1. Lawrence: Schiefelbusch Life Span Institute, University of Kansas.
Thompson, B., Wickham, D., Ault, M.M., Shanks, P., Reinertson, B., Wegner, J., & Guess, D. (1991). Expanding the circle of inclusion: Integrating young children with severe multiple disabilities. Montessori Life, 1, 11-15.
Thompson, B., Wickham, D., & Wegner, J. (1991). A qualitative research approach for investigating and evaluating an emergent early childhood inclusion model for children with severe disabilities in a Montessori preschool. Kansas Early Childhood Research Institute on Transition, Project 2.2, Working Paper No. 2. Lawrence: Schiefelbusch Life Span Institute, University of Kansas.
Thompson, B., Wickham, D., Wegner, J., Ault, M. M., Shanks, P., & Reinertson, B. (1993). Handbook for the inclusion of young children with severe disabilities: Strategies for implementing exemplary full inclusion programs. Lawrence, KS: Learner Managed Designs.
Vandercook, T., York, J,, & Forest, M. {1989). The McGill action planning system (MAPS): A strategy for building the vision. Journal of The Association or Persons with Severe Handicaps, 14(3), 205-215.
Wegner, J. (1989). Opportunities for communication intervention with preschool children with severe disabilities. Unpublished manuscript, Department of Speech, Language and Hearing, University of Kansas, Lawrence.
Wegner, J. (1991). From classroom to classroom: New ways to interact. Unpublished doctoral dissertation, University of Kansas, Lawrence.
Whitehead, L., Deiner, P., & Toccafondi, S. (1990). Family assessment: Parent and professional evaluation. Topics in Early Childhood Special Education, 10(1), 63-77.
Wickham, D, (1993). An investigation of video based for paraprofessionals in inclusive classrooms. Unpublished doctoral dissertation, University of Kansas, Lawrence.
York, J., Vandercook, T., Caughey, E., & HeIse-Neff, C. (1988). Does the “Integration Facilitator” facilitator integration? Minneapolis: University of Minnesota, Institute on Community Integration
This feature: Thompson, B.,
Wickham, D., Wegner, J., & Ault, M. (1996). All children should know
joy: Inclusive, family-centered services for young children with
significant disabilities. In D. H. Lehr & F. Brown, (Eds.), People with
disabilities who challenge the system (pp. 23-55). Baltimore, MD:
Brookes Publishing Company