

































Although many agree youth would be better served by the strengths-based resiliency paradigm, it is much harder to actually shift from focusing on the problems that placed a youth at risk to focusing on the strengths a youth has developed to handle the problems. The co-director of Project Resilience considers how challenging such change can be and offers suggestions for meeting the challenge.
As ideas go, the concept of paradigm shift is “in”. Everywhere educators, preventionists, clinicians, and policy makers are decrying the drawbacks of an “at-risk” paradigm for understanding, serving, and programming for children and youth. The alternative they advance is a resiliency model that breaks with a long tradition of research and practice emphasizing problems and vulnerabilities in children, families, communities, and institutions burdened by adversity. Instead, the resiliency model credits people with the strengths and potential to recover and bounce back from hardship. It vests power in them to help themselves and casts professionals as partners rather than as authorities, initiators, and directors of the change process.
I agree. An important part of our own work at Project Resilience has been to develop a resilience paradigm and to advocate for a shift away from the risk paradigm. At the same time, I have learned from our experience training hundreds of teachers, school and agency administrators, counselors, therapists, youth workers, and others that paradigm shifts are much more easily discussed than accomplished. Resistance is both natural and to be expected. The case of Anita, a 14-year-old student in an inner-city junior high school, illustrates the nature of the task.
Case example
Upon entering junior high school, Anita was immediately identified as an
at-risk student. She was brought to the attention of the guidance office
and the special education screening team. She was disruptive in class,
frequently calling out and making inappropriate remarks. All of her
academic skills were two to three years below grade level. Her school
record did not indicate a home address or the name of her father. Her
mother, who was a teenager when Anita was born, was addicted to crack
cocaine. Anita was frequently absent or late to school. Notes sent home
about her absences, her behavior, and her poor academic work were
unanswered.
This recitation of “facts” is the data usually marshaled by the risk paradigm and is typically used to draw conclusions. By documenting one problem after the next, the paradigm gives the impression of a teenager who is well on her way to repeating mistakes her mother made. It predicts that Anita is more likely than not to drop out of school because she is academically deficient and behaviorally and emotionally impaired. With few skills and little idea of a work ethic or the rules of the marketplace, she will be pushed to the margins of society. According to the risk paradigm, little in her past gives a reason to be hopeful about her future.
A resiliency paradigm comes to an opposing conclusion, not by denying the facts cited by the risk paradigm, but by looking at another part of the picture. For instance, resiliency thinkers point out that at home Anita takes care of both her mother and her brother. Because her mother resists treatment, Anita escorts her to the drug treatment center, often waiting many hours for her mother to be seen. She also goes along to the supermarket to be sure that her mother is buying food rather than getting sidetracked and spending her money on drugs.
Anita cooks and prepares meals for her brother. When there is not enough food to go around, she cuts down on her own meager portion so that he will not be hungry. She insists that he attend school, even when she does not. Anita has woven a safety net for herself by cultivating a relationship with her Aunt Edith. She goes to Edith’s house with her brother whenever her mother disappears or brings home a man who is frightening.
In considering these “facts,” as well as Anita’s school records and psychological and educational assessments, a resiliency paradigm holds out hope for Anita. It views her as someone with inherent strengths and the capacity to direct her future provided she is given the right support (e.g., skilled mentoring, quality compensatory education, and integrated social services). Specifically, she is a mature individual – even wise beyond her years. She is moral and has a deep sense of obligation to her family. She is self-sufficient and has considerable common sense.
In the training I have conducted, I have tried to instill doubts about the risk paradigm by introducing this type of positive information. I have tried to convey a sense of hope to those who would see Anita exclusively in terms of her problems and envision a scenario of doom for her. I have encouraged participants entrenched in the risk paradigm to broaden their perspective and to consider information that is normally omitted in risk assessments. I have not always been successful. On the contrary, I have had to learn and understand what I was up against.
Impediments to change
Shifting one’s paradigm requires personal change, and personal change
requires hard work. Consider how difficult it is to make even small
personal changes. How often have you vowed not to blow up at your
teenager only to find yourself in that very act the next day or the next
hour? Or how often have you vowed to begin a diet, start exercising, put
your credit card away, or stop procrastinating?
Compared to the difficulty of changing behaviors such as these, shifting one’s paradigm is a different order of magnitude. Paradigms are not overt behaviors that you are aware of, such as eating too much, exercising too little, or flying off the handle when you should be understanding and patient. Paradigms are deeply embedded in the self. As Steven Covey (1989) explains, a paradigm is a map inlaid in the mind which determines the way you see the world. Paradigms are conditioned by your inborn temperament, upbringing, family, friends, colleagues, schooling, and work environment. Rooted as they are, paradigms are seldom scrutinized or questioned. Rather they are accepted and drive the assumption that what you are seeing is a correct representation of reality. They preclude other people’s realities. When contradictions arise in an encounter with someone else’s paradigm, they are dismissed as inaccuracies, misperceptions, or mistakes. The whole process repeats itself again and again without notice. It is not easily interrupted.
New information does not change paradigms. Training in skills and techniques does not change paradigms. And telling others about a new paradigm in the hope that they will give up theirs and adopt yours does not often work either. As Bonnie Benard (1993) has noted, changing paradigms requires nothing less than changing people’s hearts and minds. In our attempts to do that through Project Resilience, I have identified three specific obstacles that often stand in the way. I describe them below and make suggestions for overcoming each.
1. The distance between the resiliency
and risk paradigms, as each one is typically described, is too great for
people to cross comfortably.
The resiliency paradigm is often portrayed as the opposite of the risk
paradigm. Therefore, for the resiliency paradigm to be accepted requires
the unlikely event that people will stop believing that the children and
youth they see in their offices, classrooms, and agencies each day have
been severely damaged by the hardships they face. Instead, they will
begin thinking that the damage in these children and youth is not as
significant as their strengths and resources that had previously been
ignored.
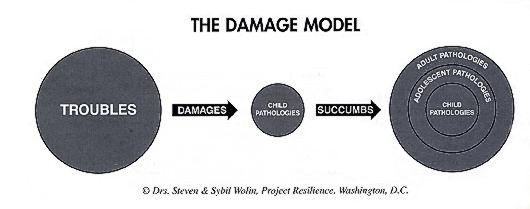
I believe that presenting the resiliency paradigm in this way is a misrepresentation and oversimplification that stirs up resistance rather than paves the way to change. A more accurate representation is that the risk paradigm, which I have called the Damage Model, and the resiliency paradigm, which I have called the Challenge Model, complement one another.
The Damage Model portrays the harm that troubled circumstances among families, communities, and societies can inflict on children. It paints children as passive and without choices or the ability to help themselves. As a result, the best they can do is cope with hardship. Over time, coping takes its toll and gives way to pathology. As the process continues, pathologies are layered upon pathologies, and the child becomes an adult with serious and often irreversible problems.
The Challenge Model starts with the same sequence. It does not require downplaying or overlooking the deleterious effects of hardship. It does, however, add another dimension to the risk story. In the Challenge Model, hardship is not only destructive but is also an opportunity. Children are wounded in the Challenge Model, as they are in the Damage Model, and they are left with scars as adults. But their troubles also challenge them to experiment and respond actively and creatively. Their preemptive responses, repeated over time, become incorporated into the self as lasting resiliencies.
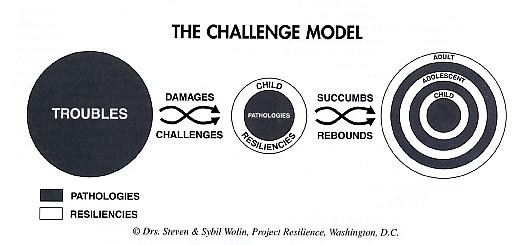
Seen from the perspective of the Challenge Model, hardship has a paradoxical effect, simultaneously causing strength and weakness. In our workshops, I have found that this notion of paradox is more easily accepted than the idea of dropping the risk paradigm completely and then working only with children who have been harmed on the basis of their strengths alone. I also believe that a paradoxical formulation, in contrast to the either/or alternative of risk versus resiliency, is more clinically accurate and responsible.
2. Compared to the resiliency paradigm,
the risk paradigm carries considerable authority that is difficult to
question or deny.
The risk paradigm is based in a long and venerable tradition of research
and practice. It stems from a medical model that seeks to identify and
eradicate the cause of physical diseases. The fields of psychiatry and
psychology extended this model from diseases of the body to disorders of
the mind. Its medical roots lent particular authority to the innovation.
Since the 1940s, when Rene Spitz (1945) first investigated hospitalism in institutionalized infants, researchers have been studying the specific disorders of the mind associated with stress and hardship in early childhood. They have uncovered the myriad ways that children's psyches can be harmed by disruptions in the functioning of their parents, families, and communities. Their work has filled libraries with data on the maladies that beset children with schizophrenic mothers, divorcing parents, alcoholic fathers, handicapped siblings, premature separations, and other similar traumas. In conjunction with clinical observations of the ill, this work is the basis of the Diagnostic and Statistical Manual (DSM-IV), which sets the standard and provides the vocabulary for diagnosing mental illness. It is hundreds of pages long and replete with categories, subcategories, flow charts, and axes.
As worthy as the investigation and identification of pathology have been, this endeavor has been one-sided, painting a distorted picture of human frailties and vulnerabilities and the insufficiencies of children to master their problems. The resiliency model, which fills in the picture, is a relative newcomer that is not yet developed enough to balance the distortions of the risk paradigm. Less than two decades old, it lacks the aura of legitimacy that history, research, and a medical background bestow upon the risk paradigm. Next to the risk lexicon, a resiliency vocabulary is scant and pallid. The paradigm itself is only just beginning to enter the clinical arena.
As a result, the resiliency paradigm is no match for the risk paradigm. Professionals feel that they have entered alien territory when they talk about inner strengths, protective factors, and the human capacity to repair from harm. They grope for words and fear sounding unschooled and naive when they replace pathology terminology with the more mundane vocabulary of courage, resourcefulness, hope, creativity, competence, and the like. Putting it all together, many prefer the familiarity and safety of the risk paradigm to the struggle of adopting a new mode of thinking. I believe that the struggle can be tipped in the other direction by offering a systematic, developmental vocabulary of strengths that can stand up to the pathology terminology that is standard in the field. Our own work has taken that direction. I have also found that some of the skepticism that is typically associated with the resiliency paradigm dissipates with information about the growing and promising field of resiliency research.
3. Talking about strengths in children
who are suffering provokes moral hesitations.
As sentient beings, people are more apt to think in terms of risk rather
than resiliency. Professional adults as well as lay people feel a
natural protectiveness toward children. Their small size, their
weaknesses and dependencies, and their injuries stir people’s deepest
sympathies. Innocent children who are needlessly hurt ignite feelings of
moral outrage. It is an appalling spectacle when they are homeless,
hungry, abused, or uneducated. In the face of such suffering, talking
about their strengths seems all wrong. This sense of incorrectness
stands in the way of widespread acceptance of a resiliency paradigm.
Feeling like they are on shaky moral ground, people retreat to the
safety of the risk paradigm and are reluctant to move out of its
enclosure.
In my workshops, I have found that the most effective way of lowering this resistance is by discussing it directly. The interchange is usually thoughtful and sobering, encouraging participants to examine and question, some for the first time, the paradigm that governs their work.
I have approached the topic in several ways. One of the most successful has been to ask workshop participants to view Salaam Bombay, a movie about Krishna, a young Indian boy who has been abandoned on the streets of Bombay. His trials and pains are monumental. They can be discussed without inhibition. His strengths and integrity of character – which are equally compelling – cause conflict. On the one hand, participants see the strengths and want to acknowledge them. But on the other hand, they fear that mentioning the strengths of children who suffer will dampen the moral outcry the movie is meant to rouse.
I use this conflict as a jumping-off point for discussing the basic underlying issue. Do we become party to the world's injustice by focusing on Krishna’s strength rather than taking action or advocating for change on his behalf? Does an emphasis on strengths in children of hardship dilute society’s obligation to help disadvantaged populations?
Although we rarely reach clear answers, an open airing of these questions at least begins the process of opening people’s minds and hearts. In the course of the discussion, I have found that most participants become curious about their own paradigms and the reasons that keep them in place. More than a few reach the conclusion that while talking about resilience in children of extreme hardship can go against the grain, it can be done responsibly, and it can result in benefits to children.
A call for shifting paradigms
Traditionally, the fields of education, prevention, and therapy for
children who struggle with hardship have been dominated by an at-risk
paradigm. The results of this approach have been disappointing to
professionals and the public alike. As a result, from all quarters,
there are urgings for something new and better. The most frequently
discussed alternative is a resiliency paradigm, which honors the
strengths of children and youth and their capacity to recover from
hardship. I join those who are calling for this shift. At the same time,
I have seen that the expectation that people can shift easily from one
paradigm to another is naive. Therefore, trainers and supervisors who
wish to encourage change in the direction of the resiliency paradigm
need to understand the nature of the resistances and what can be done to
reduce them.
References
Benard, B. (1993). Turning the corner from risk to resiliency. Portland, OR: Northwest Regional Educational Laboratory.
Covey, S. (1989). The seven habits of highly effective people: Powerful lessons in personal change. New York: Simon & Schuster.
Spitz, R. (1945). Hospitalism: An inquiry into the genesis of psychiatric conditions in early childhood. The Psychoanalytic Study of the Child, 1. pp. 53-74.
This feature: Wolin, S. (1999). Easier said than done: Shifting from a risk to a resiliency paradigm. Reaching Today’s Youth, 3, 4. pp. 11-14.