



































Introduction
Oak Hill Boys Ranch was established in 1961 in Alberta, Canada. It serves as a highly comprehensive residential treatment center for 1116 year old male youth. Young persons who are referred to Oak Hill Boys Ranch require residential treatment services for problems associated with trauma related to neglect and/or physical, emotional and sexual abuse.
Oak Hill Boys Ranch decided to embark on an initiative to reduce the use of restrictive procedures, primarily physical interventions. Physical restraint and physical intervention are terms often used interchangeably; however they have very different meanings.
Physical restraint refers to a specific act of physically holding another person, restricting and limiting their movement to prevent harm to themselves or others. Physical intervention includes all direct contact with the young person with the intention of creating safety. For example, physical intervention includes physical restraint as well as less intrusive interventions such as guiding a young person from one place to another (escorts) or escaping from the grasp of a young person (personal safety).
Often the development and implementation of initiatives which lead to changes in organisational policy and practice are a result of serious crisis. The changes at Oak Hills were put into place due to the serious injury of a young person and also due to a questioning about the therapeutic effects of restraint practice. This paper is drawn from a larger report and comprehensive literature review concerning the use of restraint. It outlines some of the data collected at Oak Hills concerning the use of restraint and presents a model for changing practice.
Therapeutic effects of restraint practice
The majority of academics, managers and practitioners who are involved in child protective services would agree that implementing an organisational goal to reduce the number of physical interventions requires little justification.
Furthermore, the use of physical restraint has been questioned on some of the following therapeutic grounds:
We know that restraint can be very traumatic not only for young people and staff who are involved but also for youth who may witness the act. According to research (Hobbs et al., 1999; Fox, 2004), trauma-specific re-enactment may occur when young persons are placed in restraints. That is, they often relive traumatic events from their past during a restraint. Perceptions of intimidation, forced compliance or physical dominance by the young person involved mirror the lesson they learnt while being abused when younger. We often witness young people who become increasingly fearful, angry and aggressive when restrictive techniques are applied, stemming from a history of trauma. Given this, our goal was to provide young people with an alternative model of healthy negotiation, therapeutic assistance and self-control.
In contrast to abused children, Hodas (2004) concludes that young people who suffer neglect seem to have difficulties decoding and understanding emotions across the spectrum. Often, these young people expect conflict/confrontation from every social encounter which often leads them to take an aggressive stance, or, alternatively, to withdraw. These findings reinforce the theory that abused or neglected young people are more attuned to anger, or what looks to them like anger, in others, bringing about feelings of trauma from the restraint process. Hodas (2004) writes that
– we need to appreciate the fact that, even when implemented properly and safely, restraint(s) are intrinsically traumatic and humiliating to most children. Restraint, in particular, has the capacity to re-traumatise children, embitter them, (and/or) undermine therapeutic relationships (Hodas, 2004, p. 12).
In order to investigate further the way in which restraints were occurring at Oak Hills, it was decided to monitor their frequency over an eight-month period.
Frequency of restraints
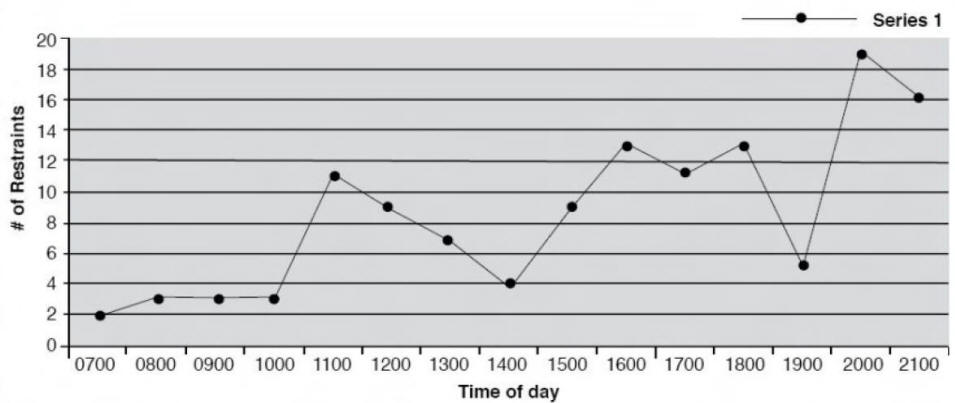
In reviewing the frequency of restraints, with the time of day, for the period of April to November, 2006 therewere some interesting data points. The three peak times of day when restraints occurred most frequently were between 11:00 a.m. and 11:59 a.m.; 4: 00 pm and 5:59 p.m. and 8:00 p.m. and 9:59 p.m. The first peak occurred after the residents had been in school since 9:00 a.m., after their last class in the morning. Given that the majority of the residents have cognitive deficits or a diagnosis of ADHD, having been engaged in class room activities for more than two hours, it would make sense that there would be an escalation in challenging behavior.
The second and third peaks, where restraints occur more frequently, account for 61 per cent of the restraints in the eight-month period. During the second peak of the day, the residents have an hour of free time which leads into the supper hour and clean up. During the third peak of the day, the residents have returned from evening activity and are typically having showers and getting ready for bed.
Although there are likely a multitude of factors that contribute to escalation of challenging behaviour which lead to restraints during these times, there are two common features. First, there appears to be limited structured activity. The residents were engaged in free play or were being organised in ways where they were not all engaged in an activity. For example, only two residents were able to use the showers at one time and often other residents are left waiting to complete their routines. Secondly, the residents were engaged in activities in their residences.
Three of the residences have between eight and twelve young people. Grouping these young people with their various challenges into a single environment, and who then have competing interests are sure to contribute to escalating challenging behaviour.
The times when restraints occurred least often were during structured organised activities. These included:
Future directions for practice at Oak Hill
In response to the data analysis, Oak Hill Boys Ranch adopted a six-stage process for administration and application of restraint reduction drawn from the work of Haimowitz et al. (2006).
1. Leadership in organizational change.
Haimowitz et al. (2006) suggest that to be successful, efforts to reduce restraints must start at the level of the Executive Director and other executive staff. Leaders should take an active and routinely visible role in announcing and implementing a plan to reduce the use of restraints. A key component of this strategy must be the assurance of the oversight of every restraint by the executive staff, including frequent communications in an effort to change traditional staff practices. Furthermore, an agency must create an environment that is very supportive and appreciative of its staff. Staff must believe they are supported by managers in their jobs and understand they have a voice in the process (Johnson 2004).
2. The use of data to inform practice.
Data should be collected and used in a non-punitive manner to facilitate awareness among staff members as to how the facility uses such interventions. The idea is to promote successes and look at areas where improvements are being made so that staff members can identify what is working and build on those successes.
Haimowitz et al. (2006) suggest that facility data collection should include the following: rates of restraint (episode and duration) per six-month period, broken down by unit and (client) characteristics; trends in restraint use, and comparisons in rates and trends between our facility and other ‘benchmark’ facilities. Carlson (2004) suggests tracking where, when and with whom restrictive techniques were more likely to occur. Once trends are determined, modifications to programme structure during these times may occur. Fulmore (2004) adds the use of data to ascertain seasonal and temporal cycles in behaviour management and subsequent allocation of increased resources during the most needed times.
3. Staff development
Staff training is imperative. As Haimowitz et al. (2006) state:
Efforts to reduce restraints are most successful in facilities where policy, procedures and practices are based on the principles of recovery and the characteristics of trauma-informed systems of care. This training should integrate trauma-informed care, the development of therapeutic relationships, value clarification, cultural competence, the use of language, individualised care planning skills and the importance of the inclusion of service users in their care planning for restraint reduction efforts (Haimowitz et al. 2006, p.26).
It is also suggested that training on critical incident report writing is implemented. Training on incident reporting should include definitions review, reporting guidelines and documentation procedures to promote a consistent, reliable measurement of incidents, as reported by commentators such as O’Brien (2004). All of the literature reviewed indicated that it is necessary to provide a training curriculum that supports the reduction of restraints. It is imperative to the success of any initiative that training is comprehensive, not only focusing on proper restraint techniques but also on therapeutic crisis intervention (Colton, 2004). We recognise that during emergency situations, restraint may become a necessary intervention to prevent harm. However, implementing safe interventions in a therapeutic manner must ensure that restraint is truly a last resort, used only in response to imminent danger to the child or others, when less restrictive therapeutic interventions have failed. In doing this we need to provide staff with the support and training to assist them in carrying out their work in a manner that informs them of what to do, not simply what not to do (Hart & Howell, 2004).
4. Use of Preventative Tools
Haimowitz et al. (2006) outline the following tools as being necessary to prevent and reduce restraints:
5. Supporting advocacy in the residential treatment setting
Involving clients’ family members, child advocates, children’s service’s workers, psychologists, psychiatrists, teachers and other members of the young person’s community in ongoing treatment issues can have a powerful impact as a prevention strategy to reduce the use of restraint. The presence of these stakeholders sends the message that the young person is supported in their efforts to utilise alternatives to violence and can serve as an ongoing reminder of treatment goals. Colton (2004) highlights factors that can enhance communication and involvement of stakeholders. This includes informing the stakeholders of the organisation's policy and when these interventions are used, including an explanation of why the intervention was necessary.
Staff interact with the client to ensure they are not isolated during the intervention and staff are responsive of the client's need to interact and reintegrate back into milieu after the intervention (Colton, 2004, p7).
6. Debriefing tools
Staff require support immediately following episodes of crisis and challenging behaviour. Haimowitz et al.(2006) suggest that debriefing activities be standardised throughout a facility, and integrated into policy and procedure. They identify two distinct debriefing activities. The first activity should immediately follow the event and should be led by supervisor or other senior staff person who was not involved in the event. The purpose of this is to confirm safety of all involved parties, review documentation, interview staff and others who were present and assist in returning the unit to the pre-crisis milieu (Haimowitz et al. 2006). Colton (2004), notes that
debriefing with the client helps the client reconnect with staff, peers and the milieu. It also provides an opportunity to reflect on the behaviours that led to the intervention and to identify coping strategies and behaviours that can be used in the future ...(taking) into consideration the individual's maturation and ability to make use of the process... also a need to process the event with staff particularly around their feelings, reactions and safety, as well as examining the situation to determine what worked or didn't work (Colton, 2004, p.7).
The second debriefing activity is more formal and should occur a few days later, attended by a predetermined review committee which may consist of the facility executive, psychologist, supervisor and other residential staff member. The purpose of this meeting is to look at root causes, review and analyse events, and identify what can be changed to avoid an event in the future. It also helps to ensure that, as much as possible, trauma is mitigated for all involved parties (Haimowitz et al.,2006). The inclusion of the client's perspective is critical. The facility may appoint a staff advocate to present the young person's perspective.
Crisis management system and staff training
Organisations have a responsibility not only to provide the best therapeutic care and therapeutic services to young people and their families, but also to ensure that practitioners have the best skills and systems in place to optimise safety and therapeutic care. Organisational policy, procedure, and practice need to optimise both client and staffing resources to ensure there is the best crisis management system in place in order to work effectively through crises that have the potential to result in physical interventions. It is important that residential treatment programmes take a comprehensive approach to crisis management through ensuring staff are well qualified, well trained in the best models available and operate a consistent crisis management system.
Conclusion
This paper was drawn from a larger report which has committed Oak Hill Boys Ranch to a comprehensive initiative that will review and revise policy, procedure and practice to minimise the utilization and application of restraint within our residential centre. In this paper, we have presented definitions of physical restraint and physical intervention, our rationale for restraint reduction, a brief analysis of physical restraint practices, and a process for the implementation of new policy, procedure and practices to support better crisis management. It is hoped that by sharing our experiences, some of the valuable lessons we learned in our review may be of assistance in the wider Child and Youth Care field.
References
Carlson, S. (2004). Reducing reliance on restrictive techniques. Residential Group Care Quarterly. 4(4), 1-3.
Colton, D. (2004). Checklist for assessing your organisation's readiness for reducing seclusion and restraint. Staunton, VA: Commonwealth Center for Children and Adolescents.
Fulmore, D. (2004). Best practices in behavior management issues: Third Nation report card. Residential Group Care Quarterly. 4(3). 10-11.
Fox, L. (2004). The impact of restraint on sexually abused children and youth. Residential Group Care Quarterly. 4(3), 1-5.
Hart, D. & Howell, S. (2004). Report on the use of physical interventions across children's services. London: NCB.
Haimowitz, J.D. Urff, J. & Huckshorn, K.A.(2006). Restraint and seclusion – A risk management guide. Alberta: National Association of State Mental Health Program Directors. Accessed on 27th May 2006 at www.nasmphd.org.
Hobbs, G. F., Hobbs C.J. & Wynne, J.M. (1999). Abuse of children in foster and residential care. Child Abuse and Neglect, 23(12), 1239-1252.
Hodas, G. (2004). Is restraint and seclusion a therapeutic intervention or therapeutic failure? Residential Group Care Quarterly. 4(3), 11-15.
Johnson, J. H. (2004). Is becoming restraint and seclusion free a realistic goal for residential providers? Residential Group Care Quarterly. 4(4), 10-12.
Miller, J. A., Hunt, D. P., & Georges, M. A. (2006). Reduction of physical restraints in residential treatment facilities. Journal of Disability Policy Studies. 16(4), 202-208.
O'Brien, C. (2004). Best practices in behavior support: Preventing and reducing the use of restraint and seclusion. Residential Group Care Quarterly. 5(2), 14-15.
This feature from the Scottish Journal of Residential Child Care, Volume 8 No 1 February/March 2009, pages 62-69