



































Current policy and practice in children's mental health recommends family centered, community-based systems of care that keep children with their families while receiving mental health treatment, rather than removing them from the natural contexts of their family, community, and cultural group. System of care principles also feature individualized services and models of service delivery that wrap services around families as well as a view of family members as partners actively participating in decision-making about their children's treatment.
Despite these advances in community-based services, there are still significant numbers of children who are placed out-of-home to receive treatment. In out-of-home treatment, the principles of family-centered services may be less central and parents may find it difficult to maintain active participation in their children's treatment. For example, residential programs often use points and levels systems as a therapeutic technique. Under such systems, the acquisition of privileges is conditioned on positive behavior. Parent-child contact may be considered as one of these “privileges", with the result that contact may be denied at any time.
In 1996 and 1997, we conducted a series of focus groups with family members and residential treatment providers. Family members reported that in many residential treatment centers, group homes, and residential facilities, their contact with their children was limited by program policies and staff practices. For example, many parents reported that they were not allowed to have contact for an initial period (frequently 1-4 weeks) after admission to allow the child to “adjust" to the new environment. Even after this settling-in period, parents reported that agency policy limited visits at the facility, day visits, and home visits as well as telephone contact with their children. Residential program staff confirmed that these practices were common in the facilities they represented.
Such limitations on parent-child contact are a concern in the light of research findings related to attachment theory and the importance of preserving children's attachments as a foundation for the capacity to form caring relationships throughout life (Bowlby, 1988). Further, there is some evidence that maintaining parent-child relationships during out-of-home care facilitates child well-being and more rapid family reunification (Davis, Landsverk, Newton, & Ganger, 1996).
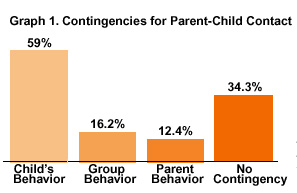
These emergent themes were used as a framework for the development of a larger survey designed to examine the experiences of families participating in their children's mental health treatment, particularly those receiving services out-of-home. A sample of 105 parents with children receiving mental health treatment in residential care facilities, group homes, and psychiatric hospitals or units responded to our survey about their experiences with limitations on parent-child contact. Fifty-seven percent of respondents said that when their child first entered the out-of-home placement, contact was limited for an initial period of adjustment. Fifty-three percent of respondents reported that contact with their children was governed by a levels system. Levels systems were used across treatment settings. Parents whose children were in placements that had a levels system were significantly more likely to have contact limited for an initial period of adjustment, but initial contact was also limited in programs that did not have a levels program. Most families reported that contact was predicated on the child's behavior (59%), but facilities also used unit or group behavior (16.2%) and parental behavior (12.4%) as criteria (Graph 1).
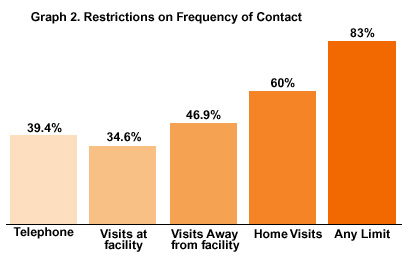
According to VanderVen (1995) the withholding of activities that are at the core of treatment (such as caregiver contact and visitation) “is probably the most frequent–and the most misinformed–misuse of points and levels [systems]" (p. 356). Withholding contact is destructive to the child's relationships with and commitment to caregivers and agency staff (Graph 2).
The practice of withholding contact may stem from underlying agency beliefs that caregivers are the cause of their child's problems, beliefs that often divide caregiver, agency, and child. One respondent to our survey wrote,
She needed time to “adjust" ... they used the time to teach her that I had caused her problems ...
Another wrote,
Do not underestimate the power of the bond between child and family even when it appears dysfunctional. Do not restrict contact between family and child when [the] child is diagnosed [with] Attachment Disorder – I felt I was “pathologized" as “enmeshed" when I protested [after] 2 months total [of] no contact."
In contrast to practices that limit parent-child contact, a large body of research has shown that ongoing contact with caregivers is related to positive behavior of children in care, the child's ability to adapt to care, and more rapid family reunification in foster care (Davis, Landsverk, Newton, & Ganger, 1996; Noble & Gibson, 1994; Tam & Ho, 1996). Logically, if the ultimate goal of residential treatment is to return the child to the family, then ongoing contact is necessary (Thomlison et al., 1996).
In addition, restrictions are different for children hospitalized for the treatment of mental illnesses then for those hospitalized for the treatment of physical illnesses. Today, most hospitals not only allow, but encourage parental contact with a child who is to have her appendix removed, but our results show that many hospitals, residential treatment centers, and group homes have rigid rules regarding contact with a child who is receiving mental health treatment.
From our focus groups and survey, it is clear that parents routinely experience limitations in contact with their children. Caregivers' words indicate that there is much work to be done to make out-of-home treatment family-centered, to reduce the stigma associated with placing a child out of home, to build specific supports for increasing parent participation, and to value the critical significance of parent-child contact. Caregivers' words say it best.
Caregivers want to feel respected:
"Honor the parents who suffer chronic grief and stress over the loss of their child."
Caregivers ask for specific help with contact:
"Treatment facilities need to be flexible in scheduling, especially when parents work and/or live out of town."
And finally, parents emphasize the value of contact with their child:
"Parents should be allowed to be as involved in their child's care in the same way as parents of physically ill children."
"Frequent contact with the child, program staff, program psychiatrist, clinician, caseworker is a must". Remember that nobody knows your child as well as you and that subtle changes can be picked up more quickly by the parent and not always by the staff."
References
Bowlby, J. (1988). Developmental psychiatry comes of age. American Journal of Psychiatry, 145, 1-10.
Davis, I.P., Landsverk, J., Newton, R., & Ganger, W. (1996). Parental visiting and foster care reunification. Children and Youth Services Review, 18(4/5), 363-382.
Noble, D.N. & Gibson, D. (1994). Family values in action: Family connectedness for children in substitute care. Child and Youth Care Forum, 23(5), 315-328.
Tam, T.S., & Ho, M.K.W. (1996). Factors influencing the prospect of children returning to their parents from out-of-home care. Child Welfare, LXXV(3), 253-268.
Thomlison, B., Maluccio, A., Abramczyk, L. (1996). The theory, policy, and practice context of family reunification: An integrated research perspective. Children and Youth Services Review, 18(4/5), 473-488.
VanderVen, K. (1995). “Point and level systems": Another way to fail children and youth. Child and Youth Care Forum, 24(6), 345-367.
This feature: Acknowledgements to Focal Point